

Gurwin Healthcare System has announced the availability of 18 newly built studio apartments in its Gurwin Jewish ~ Fay J. Lindner Residences assisted living community. The construction of the new studios marks a new choice option for the 210-luxury apartment community, located on Gurwin’s lush 36-acre Commack campus, and comes in response to market interest for more streamlined residences at a lower price point.
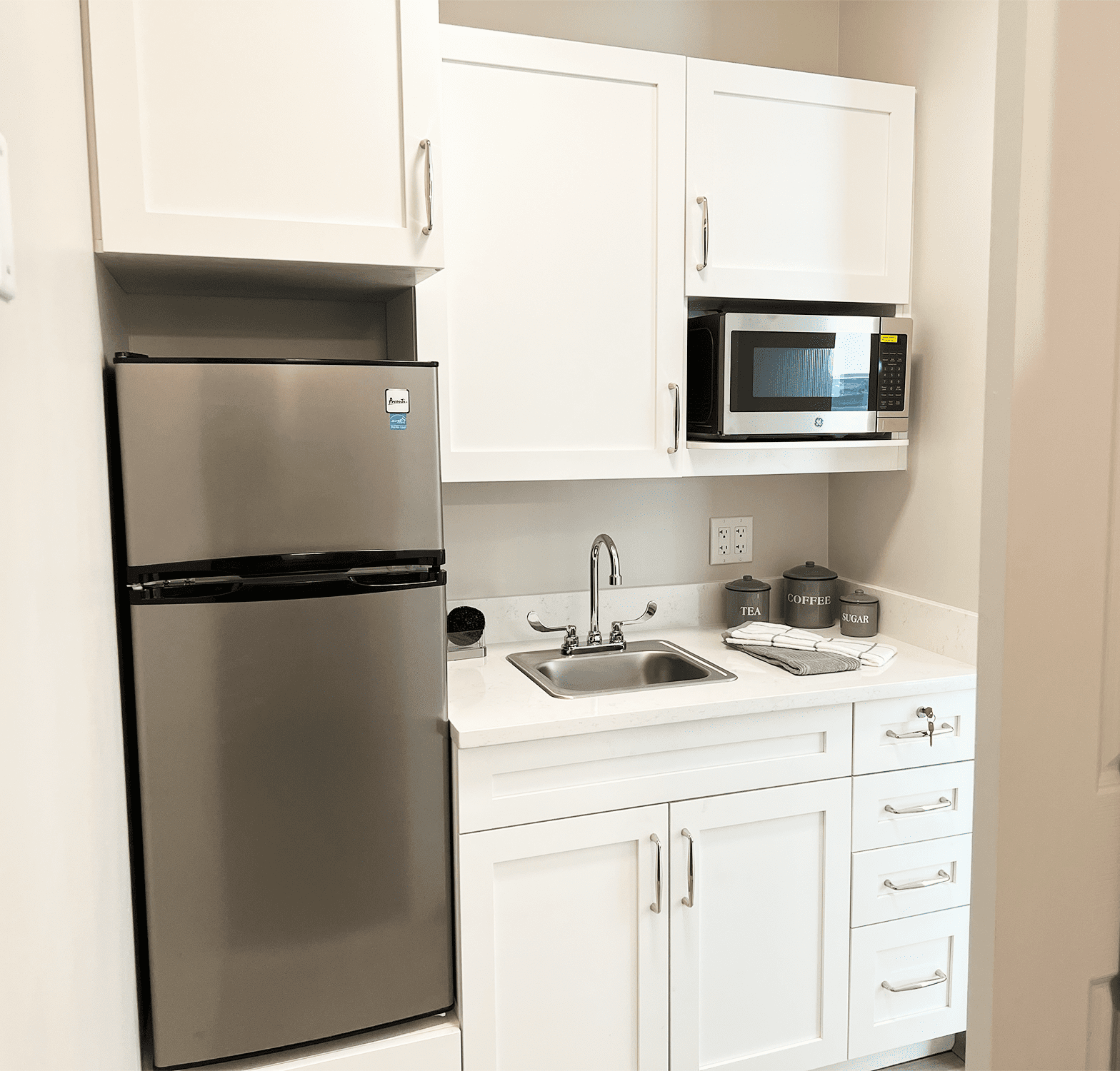
Ranging in size from 241 to 278 sq. ft., the upscale studios feature dual living/sleeping areas, a kitchenette with stainless steel appliances, spacious closets and fully ADA-equipped bathrooms. Large windows welcome natural sunlight and several studios feature courtyard views. Pricing begins at $4950 per month and includes all utilities, as well as housekeeping and maintenance services. Other available services include personal laundry, including linens and towels, and appointment transportation. Included in the monthly fee is full access to the community’s amenities, including chef-prepared meals, scheduled social activities and local outings.
“The addition of studio apartments is an evolution of the Gurwin vision. We are pleased to have an expanded choice of senior living options to offer prospective residents,” said Stuart B. Almer, CEO of Gurwin Healthcare System. “With many already spoken for, our beautiful new studios meet the needs of Long Island seniors who desire a comfortable, smaller footprint residence within a caring, active and vibrant community.”
Gurwin’s Assisted Living community includes a formal dining room, a well-stocked library, tastefully appointed gathering areas, recreation and activity rooms, a synagogue, beauty/barber salon and rooms to host guests and family. Residents also have priority access to all levels of Gurwin’s care, including Gurwin’s rehabilitation and skilled nursing facility and on-site dialysis, home care programs and adult day care. In addition, residents enjoy the community’s manicured gardens, beautifully landscaped walking paths, and myriad outdoor activities including a shuffleboard court, putting green and LifeTrail exercise stations
About Gurwin Jewish ~ Fay J. Lindner Residences
Gurwin Jewish ~ Fay J. Lindner Residences assisted living community, located in Commack, Long Island, is part of the Gurwin Healthcare System, a renowned provider of a full continuum of healthcare and senior living services. In addition to its assisted living community, the System provides skilled nursing care, rehabilitation therapy, advanced care, ventilator and respiratory care, on-site dialysis, memory care, and palliative and hospice care, as well as adult day care programs and home care services. Skilled nursing and rehabilitation services are also available through Gurwin’s affiliate, Island Nursing and Rehab Center, located in Holtsville, Long Island. The campus is also home to Fountaingate Gardens, a newly opened 129-apartment independent living Life Plan Community for seniors age 62 and older. For more information, visit www.gurwin.org or call 631-715-8500. Follow Gurwin on Facebook (bit.ly/GurwinAssistedLiving) and on Twitter (@GurwinJewish).





















