In the UK and Europe, the term Swiss cheese has no meaning.
By Bob Lipinski
“What is a harp but an oversized cheese slicer with cultural pretensions?”
— Denis Norden, English comedy writer
“Swiss cheese” as we know it doesn’t really exist. It is a generic term often used in North America for any type of cheese, regardless of where it comes from, as long as it has a pale-yellow body and is literally full of holes or “eyes,” with a rubbery texture. And this holds true for both imported and “domestic” Swiss cheeses.
Most of the time the cheese is actually Emmentaler from Switzerland or Jarlsberg from Norway. In the UK and Europe, the term Swiss cheese has no meaning and asking for a “pound of Swiss cheese” would be the equivalent of saying, “I’d like a pound of Italian cheese” in Italy, whereby Italians would ask, “Which Italian cheese?”
Switzerland produces more than 450 varieties of cheese (mostly from cow’s milk) and they are not all called “Swiss Cheese.” Emmentaler, a cow’s milk cheese comes from the Emme Valley (near Bern), Switzerland, where it has been made since the fifteenth century. It has a pale-yellow exterior with large shiny holes and a natural edible rind; light yellow interior and is wheel-shaped. It is firm to very firm; with an almost elastic, smooth, plastic texture and slightly oily. Emmentaler is mild to full-flavored, with a sweet, fruity, nutty flavor. A younger and milder version is known as Baby Swiss. Genuine Swiss Emmentaler has the word “Switzerland” stamped all over the rind.
By the way, the holes in the cheese are produced by carbonic acid gas bubbles during fermentation or bacterial activity, which generates propionic acid and causes gas to expand within the curd also creates the holes. The bubbles are unable to escape, which is responsible for the “hole” formation ranging from pinhead size to dime or quarter size. They are sometimes made mechanically for appearance sake. Before serving the cheese, allow it to sit for 30 minutes to one hour at room temperature, which will soften the texture, release the aromas and maximize the flavor.
Now my wine recommendations:
2015 Torre Santa La Rocca “Bombino Nero” Rosé (Italy): Salmon color with an intense fruity bouquet of cherry, strawberry and melon. Dry and quite flavorful; citrus, orange and raspberries abound. Great for Sunday brunch.
2012 Château Prieurs de la Commanderie (Pomerol, Bordeaux): (80 percent merlot/ 20 percent cabernet franc). Bouquet and flavor of black cherry, plums and cedar. Medium-bodied, quite smooth and very easy to drink now or in a few years. I think of lamb chops rubbed with rosemary.
2014 Komodo Dragon “Red Blend” Columbia Valley, Washington: Quite dark with a full bouquet and flavor of black currants, black cherries, chocolate and licorice. Hints of nutmeg, cinnamon, coffee and vanilla. Pair this with a porterhouse steak.
Bob Lipinski, a local author, has written 10 books, including “101: Everything You Need to Know About Whiskey” and “Italian Wine & Cheese Made Simple” (available on Amazon.com). He conducts training seminars on wine, spirits and food and is available for speaking engagements. He can be reached at www.boblipinski.com OR [email protected].
Whether you love him or hate him, take a moment to reflect
By Michael Tessler
Michael Tessler
This piece is not an evaluation of the president’s legislative accomplishments or failures. or even his politics — but rather a reflection of the very personal impact the 44th president had on one 15-year-old boy from Port Jefferson.
It was 2008 and I was just coming of age. Then I saw him on television, delivering his iconic “Yes We Can” speech. In that moment Barack Obama instilled in me a genuine sense of hope, a firm belief that in the course of human history it is possible to make a lasting difference. His words transformed my perception of our Constitution. No longer was it a thing of antiquity, but rather something tangible, something alive, and worthy of any sacrifice to protect.
My sense of purpose and my role in our democracy cemented itself in those early days of 2008. At 15 I found myself going to school in a blazer adorned with Obama/Biden ’08 and button sporting an Afro worthy of the Jackson 5. My teachers were endlessly amused at the sight. Some of my skeptical peers would ask me: “If you’re not old enough to vote, why do you care?”
On Tuesday, Nov. 4, 2008, at 15 (and a half) I hurried back from Drama Club rehearsal with my best friend Jonathan to watch the poll results come in. This was the first election I had ever volunteered for. My family huddled around our television, my
anxieties and nerves were relentless, and then they called it — “Barack Obama has been elected the 44th president of the United States of America.” Despite having not yet lived through a full decade, tears streamed from my eyes. My country, our country, the greatest country on Earth, had just elected its first African-American president.
In that moment I saw the unending potential of America that our founders envisioned so long ago in Philadelphia. During his inaugural address, his tone changed. Like every commander-in-chief he was inheriting the weight of the most powerful office in the world. So he called upon me, as he did all Americans, to not become complacent in the future of our union — and so my work began.
Though I didn’t know it at the time, I had established what would later become known as the International Youth Congress — an organization whose aim it was to answer that question: “If you’re not old enough to vote, why do you care?”
No generation chooses to inherit the world, we just do. Despite not having a vote, our voices were no less diminished. For six years our organization grew: helping passing legislation, providing education and resources for young people around the world and eventually building a network of youth leaders from six different continents and over 20 separate countries. We were making that great hypothetical “change” possible. From as far as Rwanda, to Pakistan and Spain we gathered together to chart a common vision for the future based on our shared sense of humanity.
In these past eight years we’ve all grown up and have taken it upon ourselves to serve our communities, nation and world — whether working for the United Nations, Foundation of Economic Education, United States Senate, European Youth Parliament, International Labour Organization, the White House or this very publication. That spark would have never been lit had it not been for a certain presidential candidate with a funny name and big ears.
No legislative accomplishment or disagreement will ever measure up to the enormous inspiration Barack Hussein Obama delivered not just to me but to millions of young people around the world. His time in office has come to its constitutional conclusion, but for those whom he has inspired … we’re just getting started.
Though as I grow older my politics have changed and evolved, and we don’t always see eye to eye, I will always be grateful for that timeless creed bestowed upon a generation raised in a weary era of uncertainty — Yes We Can. Thank you Mr. President, wishing you and your family nothing but happiness in the many years ahead.
Simple lifestyle changes can make a big difference. Stock photo
By David Dunaief
Dr. David Dunaief
It seems like almost everyone is diagnosed with gastroesophageal reflux disease (GERD), or at least it did in the last few weeks in my practice. I exaggerate, of course, but the pharmaceutical companies do an excellent job of making it appear that way with advertising. Wherever you look there is an advertisement for the treatment of heartburn or indigestion, both of which are related to reflux disease.
GERD, also known as reflux, affects as much as 40 percent of the U.S. population (1). Reflux disease typically results in symptoms of heartburn and regurgitation brought on by stomach contents going backward up the esophagus. For some reason, the lower esophageal sphincter, the valve between the stomach and esophagus, inappropriately relaxes. No one is quite sure why it happens with some people and not others. Of course, a portion of reflux is physiologic (normal functioning), especially after a meal (2).
GERD risk factors are diverse. They range from lifestyle — obesity, smoking cigarettes and diet — to medications, like calcium channel blockers and antihistamines. Other medical conditions, like hiatal hernia and pregnancy, also contribute (3). Diet issues include triggers like spicy foods, peppermint, fried foods and chocolate.
Smoking and salt’s role
One study showed that both smoking and salt consumption added to the risk of GERD significantly (4). Risk increased 70 percent in people who smoked. Surprisingly, people who used table salt regularly saw the same increased risk as seen with smokers. Treatments vary, from lifestyle modifications and medications to surgery for severe, noticeable esophagitis. The goal is to relieve symptoms and prevent complications, such as Barrett’s esophagus, which could lead to esophageal adenocarcinoma. Fortunately, Barrett’s esophagus is not common and adenocarcinoma is even rarer.
Medications
The most common and effective medications for the treatment of GERD are H2 receptor blockers (e.g., Zantac and Tagamet), which partially block acid production, and proton pump inhibitors (e.g., Nexium and Prevacid), which almost completely block acid production (5). Both classes of medicines have two levels: over-the-counter and prescription strength. Here, I will focus on PPIs, for which more than 113 million prescriptions are written every year in the U.S. (6).
PPIs include Nexium (esomeprazole), Prilosec (omeprazole), Protonix (pantoprazole) and Prevacid (lansoprazole). They have demonstrated efficacy for short-term use in the treatment of Helicobacter pylori-induced (bacteria overgrowth in the gut) peptic ulcers, GERD symptoms and complication prevention, and gastric ulcer prophylaxis associated with NSAID use (aspirin, ibuprofen, etc.) as well as upper gastrointestinal bleeds.
However, they are often used long-term as maintenance therapy for GERD. PPIs used to be considered to have mild side-effects. Unfortunately, evidence is showing that this may not be true. Most of the data in the package inserts is based on short-term studies lasting weeks, not years. The landmark study supporting long-term use approval was only one year, not 10 years. Maintenance therapy usually continues over many years.
Side effects that have occurred after years of use are increased risk of bone fractures and calcium malabsorption; Clostridium difficile, a bacterial infection in the intestines; potential B12 deficiencies; and weight gain (7).
Fracture risks
There has been a debate about whether PPIs contribute to fracture risk. The Nurses’ Health Study, a prospective (forward-looking) study involving approximately 80,000 postmenopausal women, showed a 40 percent overall increased risk of hip fracture in long-term users (more than two years’ duration) compared to nonusers (8). Risk was especially high in women who also smoked or had a history of smoking, with a 50 percent increased risk. Those who never smoked did not experience significant increased fracture risk. The reason for the increased risk may be due partially to malabsorption of calcium, since stomach acid is needed to effectively metabolize calcium.
In the Women’s Health Initiative, a prospective study that followed 130,000 postmenopausal women between the ages of 50 and 79, hip fracture risk did not increase among PPI users, but the risks for wrist, forearm and spine were significantly increased (9). The study duration was approximately eight years.
Bacterial infection
The FDA warned that patients who use PPIs may be at increased risk of a bacterial infection called C. difficile. This is a serious infection that occurs in the intestines and requires treatment with antibiotics. Unfortunately, it only responds to a few antibiotics and that number is dwindling. In the FDA’s meta-analysis, 23 of 28 studies showed increased risk of infection. Patients need to contact their physicians if they develop diarrhea when taking PPIs and the diarrhea doesn’t improve (10).
B12 deficiencies
Suppressing hydrochloric acid produced in the stomach may result in malabsorption issues if turned off for long periods of time. In a study where PPIs were associated with B12 malabsorption, it usually took at least three years duration to cause this effect. B12 was not absorbed properly from food, but the PPIs did not affect B12 levels from supplementation (11). Therefore, if you are taking a PPI chronically, it is worth getting your B12 and methylmalonic acid (a metabolite of B12) levels checked and discussing possible supplementation with your physician if you have a deficiency.
My recommendations would be to use PPIs short-term, except with careful monitoring by your physician. If you choose medications for GERD management, H2 blockers might be a better choice, since they only partially block acid. Lifestyle modifications may also be appropriate in some of the disorders, with or without PPIs. Consult your physician before stopping PPIs since there may be rebound hyperacidity (high acid produced) if they are stopped abruptly.
Lifestyle modifications
A number of modifications can improve GERD, such as raising the head of the bed about six inches, not eating prior to bedtime and obesity treatment, to name a few (12). In the same study already mentioned with smoking and salt, fiber and exercise both had the opposite effect, reducing the risk of GERD (5). This was a prospective (forward-looking) trial. The analysis by Journal Watch suggests that the fiber effect may be due to its ability to reduce nitric oxide production, a relaxant for the lower esophageal sphincter (13).
Obesity
In one study, obesity exacerbated GERD. What was interesting about the study is that researchers used manometry, which measures pressure, to show that obesity increases the pressure on the lower esophageal sphincter significantly (14). Intragastric (within the stomach) pressures were higher in both overweight and obese patients on inspiration and on expiration, compared to those with normal body mass index. This is yet another reason to lose weight.
Eating prior to bed — myth or reality?
Though it may be simple, it is one of the most powerful modifications we can make to avoid GERD. There was a study that showed a 700 percent increased risk of GERD for those who ate within three hours of bedtime, compared to those who ate four hours or more prior to bedtime. Of note, this is 10 times the increased risk of the smoking effect (15). Therefore, it is best to not eat right before bed and to avoid “midnight snacks.” Although there are a number of ways to treat GERD, the most comprehensive have to do with modifiable risk factors. Drugs have their place in the arsenal of choices, but lifestyle changes are the first and most effective approach in many instances.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
From left, outgoing Secretary of the Department of Energy Ernest Moniz with BNL Laboratory Director Doon Gibbs taken at the opening of the National Synchrotron Light Source II at BNL. Photo courtesy of BNL
By Daniel Dunaief
Before Ernest Moniz ends his tenure as Secretary of the Department of Energy, he and his department released the first annual report on the state of the 17 national laboratories, which include Brookhaven National Laboratory.
On a recent conference call with reporters, Moniz described the labs as a “vital set of scientific organizations” that are “critical” for the department and the country’s missions. Experts from the labs have served as a resource for oil spills, gas leaks and nuclear reactor problems, including the meltdown at Fukushima in 2011 that was triggered by a deadly tsunami. “They are a resource on call,” Moniz said.
In addition to providing an overview of the benefit and contribution of the labs as a whole, the annual report also offered a look at each of the labs, while highlighting a research finding and a translational technology that has or will reach the market. In its outline of BNL, the report heralded an “exciting new chapter of discovery” triggered by the completion of the National Synchrotron Light Source II, a facility that allows researchers at BNL and those around the world who visit the user facility to explore a material’s properties and functions with an incredibly fine resolution and sensitivity.
Indeed, scientists are already exploring minute inner workings of a battery as it is operating, while they are also exploring the structure of materials that could become a part of new technology. The DOE chose to shine a spotlight on the work Ralf Seidl, a physicist from the RIKEN-BNL Research Center, has done with several collaborators to study a question best suited for answers at the Relativistic Heavy Ion Collider.
Seidl and his colleagues are exploring what gives protons their spin, which can affect its optical, electrical and magnetic characteristics. The source of that spin, which researchers describe not in terms of a top spinning on a table but rather as an intrinsic and measurable form of angular momentum, was a mystery.
Up until the 1980s, researchers believed three subatomic particles inside the proton created its spin. These quarks, however, only account for a third of the spin. Using RHIC, however, scientists were able to collide protons that were all spinning in a certain direction when they smash into each other. They compared the results to protons colliding when their spins are in opposite directions.
More recently, Seidl and his colleagues, using higher energy collisions, have been able to see the role the gluons, which are smaller and hold quarks together, play in a proton’s spin. The gluons hadn’t received much attention until the last 20 years, after experiments at CERN, in Geneva, demonstrated a lower contribution from quarks. “We have some strong evidence that gluons play a role,” Seidl said from Japan, where he’s working as a part of an international collaboration dedicated to understanding spin.
Smaller and more abundant than quarks, gluons are like termites in the Serengeti desert in Africa: They are hard to see but, collectively, play an important role. In the same report, the DOE also celebrated BNL’s work with fuel cell catalysts. A senior chemist at BNL, Radoslav Adzic developed a cheaper, more effective nanocatalyst for fuel cell vehicles. Catalysts for fuel cells use platinum, which is expensive and fragile. Over the last decade, Adzic and his collaborators have developed a one-atom-thick platinum coating over cheaper metals like palladium. Working with BNL staff scientists Jia Wang, Miomir Vukmirovic and Kotaro Sasaki, he developed the synthesis for this catalyst and worked to understand its potential use.
N.E. Chemcat Corporation has licensed the design and manufacturing process of a catalyst that can be used to make fuel cells as a part of a zero-emission car. This catalyst has the ultra low platinum content of about two to five grams per car, Adzic said. Working at BNL enabled partnerships that facilitated these efforts, he said. “There is expertise in various areas and aspects of the behavior of catalysts that is available at the same place,” Adzic observed. “The efficiency of research is much more convenient.”
Adzic, who has been at BNL for 24 years, said he has been able to make basic and applied research discoveries through his work at the national lab. He has 16 patents for these various catalysts, and he hopes some of them will get licensed. Adzic hopes this report, and the spotlight on his and other research efforts, will inspire politicians and decision makers to understand the possibility of direct energy conversion. “There are great advances in fuel cell development,” Adzic said. “It’s at the point in time where we have to do some finishing work to get a huge benefit for the environment.”
At the same time, the efficiency of fuel-cell-powered vehicles increases their economic benefit for consumers. The efficiency of an internal combustion engine is about 15 percent, whereas a fuel cell has about 60 percent efficiency, Adzic said.
BNL’s Laboratory Director Doon Gibbs welcomed the DOE publication. “This report highlights the remarkable achievements over the past decade of our national lab system — one that is unparalleled in the world,” he said. Gibbs suggested that the advanced details in the report, including the recognition for the NSLS II, span the breadth of BNL’s work. “They’re just a snapshot of what we do every day to make the world a better place,” Gibbs said.
While the annual report is one of Moniz’s final acts as the secretary of the agency, he hopes to communicate the vitality and importance of these labs and their work to the next administration.“I will be talking more with secretary nominee [Richard] Perry about the labs again as a critical jewel and resource,” Moniz said. “There’s a lot of support in Congress.” Moniz said the DOE has had five or six lab days, where labs share various displays with members of the legislative body. Those showcases have been “well-received” and he “fully expects the labs to be vital to the department.”
Dear Readers, Welcome to our newest column in Arts & Lifestyles! Long Island is home to many wonderful and talented artists. Each month we will feature a local artist who will share his or her favorite paintings as well as their own personal story.
’Art is not what I do, art is who I am.’ — Renee Caine‘In the Moment’
Holbrook resident Reneé Caine has shown her work around Long Island for the past 20 years, most notably with the Huntington Arts Council, East Hampton Guild, Catherine Lorillard Art Club and the Watermill Museum. For the past eight years, she has exhibited with the Setauket Artists at the Setauket Neighborhood House and is a member of LIMarts. Currently, Caine is Artist of the Month at the LIMarts latest exhibit at The Long Island Museum’s Visitors Center titled Inspired By …, which is on view through Jan. 29.
What is your background in art?
I have drawn, painted or created some form of art my entire life. I received my bachelor’s of fine arts from Dowling College with a major in art education and a master’s of arts liberal studies with an emphasis in art from Stony Brook University. I have explored all types of medium including watercolor, gouache, oil, acrylic, chalk, oil pastel, pottery, clay sculpture, printmaking, soap stone carving and bronze casting.
I taught art to grades K-12 in several districts with the last 18 years of my career teaching in the Three Village school district. When I taught, I let my students know that I was a working artist and they loved to see my work. It is rewarding to see students show up at my exhibits! I have even been critiqued by a few of them using the skills I taught them!
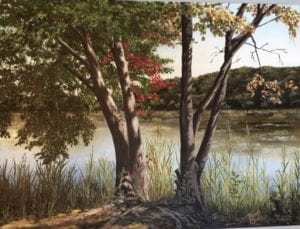
‘Peconic River’
Who influenced you to become an artist?
My grandmother was a respected watercolorist in St. Paul, Minnesota, so I think some of my talent is genetic. For years, I followed in her footsteps painting in watercolor, but now I am painting in oils.
What is your motivation?
Picasso once said his art “was like a visual diary.” That is exactly how I feel about my work. My paintings are a reflection of where I’ve been and what I’ve seen that has caught my eye or spoken to me. When I paint, I want to draw the viewer into my “Ah” moment. I am showing the viewer what caught my eye: color, light, shadow, contrast and textures in everything around us.
How would you describe your art?
I am a realist. My work is representational. I want the viewer to experience what I felt when I saw “It.” Although realistic, I still use “artistic license” to make changes. I do not try to improve on mother nature, but at times try to clean up man’s debris. My paintings are calm, restful and peaceful and I invite the viewer to step into my world to escape for a while. However, there are times that I wish to experiment with contemporary genres such as “Hello,” which won an award at a LIMarts exhibit titled I’ve Got the Music in Me.
‘Parisian Door, Number 4,’
Do you have any early memories of your art?
My first painting I ever sold was a nine by twelve oil pastel of a horse grazing in a field. I was in ninth grade when the secretary in the office wanted to buy it. She paid me $20 saying, “You will sell many of your paintings in your life, but you will always remember the first one you sold.” She was right as that experience was a wonderful incentive and affirmation for a child.
Do you have a favorite painting?
I remember the day I was in the Metropolitan Museum of Art and saw Johannes Vermeer’s “Young Woman with a Water Jug” painted in 1632. Having seen it only in textbooks, I was surprised by how small it was. Although small, I found it was powerful. Vermeer’s use of light so astounded me that it remains my favorite painting to this day.
Where is your favorite place to paint?
I am quite sure that Giverny, France, is now and will remain the most motivating place I’ve ever been. While walking through Monet’s home and gardens, I felt almost transformed to another time. As I was processing all the beauty surrounding me, I felt the enormous energy there.
What is your process when painting?
When something inspires me I take many photographs of the subject from different angles and with different lighting; then I visualize the composition in my head. It is not unusual for me to think about a painting for a couple of months before I paint it.
What is your vision for your future in art?
I feel my talent is God-given, therefore, it is my wish to develop it to the fullest. I want each painting to be an improvement over the last one. With each painting I learn something new. Growth is my quest! Keep growing, keep learning is my motto! Since I retired, I am devoting myself to my art full time and immersing myself into the art community. In the new year, I am especially looking forward to working with Neil Watson by becoming a member of the steering committee for LIMarts.
What are your other interests?
Outside of my devotion to my husband, daughter, son and three adorable grandsons, I’m an avid gardener. My property is my living sculpture. I have color from early April to late November. I have nooks, crannies and brick walkways I designed and put in myself. My vegetable garden feeds my family all summer and growing an abundance of cucumbers supplies us with pickles that we enjoy all winter. When I’m not gardening, I can be found painting in my garden! I will continue to grow as art is not what I do, art is who I am.
For many, the question of how to best care for our aging loved ones becomes a reality sooner than we think. Most people, when given the option, would prefer to age in place, remain in their homes for as long as possible receiving the care services they need in a familiar setting surrounded by family. For many, the Community-Based Long-Term Care Program, commonly referred to as Community Medicaid, makes that an affordable and therefore viable option.
Oftentimes we meet with families who are under the impression that they will not qualify for these services through the Medicaid program due to their income and assets. In most cases, that is not the case. Although an applicant for Community Medicaid must meet the necessary income and assets levels, it is important to note that there is no “look back” for Community Medicaid. What this means is that for most people, with minimal planning, both the income and asset requirements can be met with a minimal waiting period, allowing families to mitigate the cost of caring for their loved ones at home.
An individual who is applying for Medicaid Home Care may have no more than $14,850 in nonretirement liquid assets. Retirement assets will not be counted as a resource so long as the applicant is receiving monthly distributions from the account. An irrevocable prepaid burial fund is also an exempt resource. The primary residence is an exempt asset during the lifetime of the Medicaid recipient; however, if the applicant owns a home, it is advisable to consider additional estate planning to ensure that the home will be protected once the Medicaid recipient passes away.
With respect to income, a single applicant for Medicaid is permitted to keep $825 per month in income plus a $20 disregard. However, if the applicant has income that exceeds that $845 threshold, a pooled income trust can be established to preserve the applicant’s excess income and direct it to a fund where it can be used to pay his or her household bills.
These pooled trusts are created by not-for-profit agencies and are a terrific way for persons to take advantage of the many services available through Medicaid Home Care while still preserving their income for use in meeting their monthly expenses.
Functionally, the way that these trusts work is that the applicant sends a check to the fund monthly for that amount that exceeds the allowable limit. Together with the check, the applicant submits household bills equal to the amount sent to the trust fund. The trust deducts a small monthly fee for servicing these payments and then, on behalf of the applicant, pays those household bills.
As you can see, this process allows the applicant to continue relying on his monthly income to pay his bills and, at the same time, reduce his countable income amount to the amount that is permitted under the Medicaid rules. An individual who is looking for coverage for the cost of a home health aide must be able to show that they require assistance with their activities of daily living. Some examples of activities of daily living include dressing, bathing, toileting, ambulating and feeding. In fact, where the need is established, the Medicaid program can provide care for up to 24 hours per day, seven days per week.
The Community-Based Medicaid Program is an invaluable program for many seniors who wish to age in place but are unable to do so without some level of assistance.
Nancy Burner, Esq. practiceselder law and estate planning from her East Setauket office.
I’m sure we all can agree that type 2 diabetes is an epidemic that needs to be discussed again. Again, because this disease is just not going away. There are a number of different drug classes to treat diabetes, and these classes keep on growing in number and diversity; each has its merits and drawbacks. Since there are so many drugs and drug classes, you will need a scorecard to keep track.
When we talk about this disease, the first thing that comes to mind is glucose levels, or sugar, which is what defines having diabetes. However, we are going to look beyond the sugars to the nonglycemic effects.
What do I mean by this? There seems to be a renaissance occurring where there is a focus in drug trials on the treatment of diabetes complications rather than just the lowering of sugars. Some of the complications that we will investigate include cardiovascular disease and nonalcoholic fatty liver disease (NAFLD). Several drugs may reduce the risk of cardiovascular disease (CVD) mortality. Diabetes patients who have cardiovascular disease are more likely to die about 12 years prematurely (1). However, new research suggests that relatively new diabetes drugs reduce the risk of CVD mortality. These include empagliflozin (Jardiance), a sodium-glucose cotransporter 2 (SGLT2) inhibitor, and liraglutide, a glucagon-like peptide-1 (GLP1) receptor agonist. There is also a third, older drug that has shown CVD risk benefit, metformin. Though these drugs are not without their caveats. Liraglutide has also been shown to potentially reduce the risk of nonalcoholic fatty liver disease.
In fact, the American College of Physicians has recently updated its recommendations on the treatment of type 2 diabetes with oral medications (2). The first line continues to be metformin, the tried and true. The favored second-line drugs to add to metformin may be the SGLT2 cotransporter inhibitors, such as empagliflozin, or DPP-4 inhibitors, such as sitagliptin. The sulfonylureas class, such as glimepiride, and thiazolidinediones class, such as pioglitazone, are also consider second line but not as favorable. GLP1 receptor agonists, such as liraglutide, are not on the list, since they are injectable medications. There are always downsides to drug therapy, and diabetes drugs are no exception. Drawbacks include expense with newer drugs, as well as adverse side effects with all of these drugs, new and old. Though empagliflozin has been shown to reduce CVD mortality, others in the same class have been shown to increase the risk of acute kidney failure.
Before I go any further, I want to state that lifestyle modifications including a plant-based diet and exercise are likely the most powerful tools we have in treating, preventing and reversing diabetes. So, I am not a proponent of diabetes drugs. But, there are many patients who could and do benefit from drug therapy. Lifestyle modifications should always be a significant component whether on drugs or not. Recently, plant-based diets were ranked highly for treating and preventing diabetes in U.S. News and World Report, with the DASH (dietary approach to stop hypertension) diet ranked number one and the Mediterranean diet number two (3), although rankings are not the be-all and end-all. Let’s look at the evidence.
New diabetes drugs may reduce cardiovascular mortality.
Drug benefit on cardiovascular disease
As I mentioned, there are two new drugs, empagliflozin and liraglutide, and one older drug, metformin, that have shown potentially beneficial effects on the macrovascular portion of diabetes treatment and prevention — cardiovascular disease. For the longest time, most diabetes drug trials were focused only on reducing sugars, not on clinical end points.
Empagliflozin
In a the EMPA-REG OUTCOME trial, a randomized, double-blind, placebo-controlled trial, results showed that empagliflozin reduces the risk of cardiovascular mortality (heart attack or stroke) by a relative 38 percent compared to placebo in patients with type 2 diabetes and cardiovascular disease (4). There was also a 32 percent reduction in all-cause mortality compared to the placebo group. Two different doses of empagliflozin were used with similar results, 10 mg and 25 mg once a day. There were 7,020 patients with a duration of 3.1 years. Most of those in the placebo arm were on statin (cholesterol) drugs, ACE inhibitors (blood pressure medication) and aspirin.
The FDA approved this drug for the prevention of heart attacks and strokes in diabetes patients with known cardiovascular disease (5). However, the FDA advisory board only narrowly recommended the drug for this label (6). The label change is based on one trial, and the mechanism for CVD mortality reduction is unclear. However, there are several pitfalls to this study. Empagliflozin was compared to placebo, rather than the usual standard of care, and these patients had cardiovascular disease, which means that we don’t know if the benefit actually holds true in those without CVD. Interestingly, the placebo group’s HbA1C was 8.2 percent at the trial’s end, while the treatment group was reduced to 7.8 percent, neither of which is considered controlling the sugar levels. The treatment group saw a 0.5 percent reduction in HbA1C, which is not overwhelming.
In terms of adverse reactions, empagliflozin increases the risk of urinary tract infections and diabetic ketoacidosis, since sugar is excreted through the urine. In fact, the FDA warned that two drugs from the same class as empagliflozin increase the risk of acute renal failure. These are canagliflozin (Invokana) and dapagliflozin (Farxiga) (5).
Liraglutide
In the LEADER trial, a randomized controlled trial, results showed that liraglutide 1.8 mg subcutaneous injection daily decreased the risk of CVD mortality by a significant 22 percent compared to placebo plus standard care after 3 years (7). This is the highest tolerated dose. This trial involved over 9,000 type 2 diabetes patients at high risk for CVD. Liraglutide also showed a 2.3-kg (5-lb) weight reduction and 0.4 percent HbA1C drop compared to placebo by the 3-year mark. The duration of trial was 3.5 to 5 years. The most significant side effects were gastrointestinal and increased heart rate. In another study, results showed that liraglutide reduced the liver fat in 57 NAFLD patients who were not adequately controlled on metformin, insulin or sulfonylureas (8). After six months, the liver fat in these patients decreased by 33 percent. The patients also lost almost 8 lb of weight and reduced HbA1C by 1.6 percent from 9.8 to 7.3.
Metformin
In a retrospective (backward-looking) study of over 250,000 diabetes patients, there was a greater than 40 percent reduction in cardiovascular events or mortality with metformin compared to sulfonylureas (9). However, a retrospective study is not the most reliable.
Triglyceride-lowering drug reduces CVD
Fenofibrate, which had been shown not to be of benefit, may actually help reduce CVD in a specific group of diabetes patients. In a recent analysis of the ACCORDION trial, a subset of data suggests that diabetes patients with triglycerides >204 mg/dL and HDL <34 mg/dL, when treated with fenofibrate in addition to statins, saw a 27 percent significant reduction in cardiovascular events (10). This was an observational study that requires confirmation with a randomized controlled trial. Thus, there may be a use, though a narrow one, for fenofibrate.
It is potentially exciting that drugs may reduce cardiovascular mortality in diabetes patients. If you do chose one or more of these drug therapies after discussing it with your physician, remember these drugs are in addition to continuing to work on diet and on exercise — the cornerstone of therapy.
References: (1) JAMA. 2015;314(1):52-60. (2) Ann Intern Med. online Jan. 3, 2017. (3) usnews.com. (4) N Engl J Med 2015; 373:2117-2128. (5) FDA.gov. (6) Medscape.com. (7) N Engl J Med 2016; 375:311-322. (8) J Clin Endocrinol Metab. Online Oct. 12, 2016. (9) Ann Intern Med. 2012 Nov. 6;157(9):601-610. (10) JAMA Cardiology online Dec. 28, 2016.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
Born in Berlin just before World War II, Eckard Wimmer has dedicated himself in the last 20 years to producing something that would benefit humankind. A distinguished professor in molecular genetics and microbiology at Stony Brook University, Wimmer is hoping to produce vaccines to prevent the spread of viruses ranging from influenza, to Zika, to dengue fever, each of which can have significant health consequences for people around the world.
Using the latest technology, Wimmer, Steffen Mueller and J. Robert Coleman started a company called Codagenix in Melville. They aim to use software to alter the genes of viruses to make vaccines. “The technology we developed is unique,” said Wimmer, who serves as senior scientific advisor and co-founder of the new company.
Mueller is the president and chief science officer and Coleman is the chief operating officer. Both worked for years in Wimmer’s lab. Despite the potential to create vaccines that could treat people around the world facing the prospect of debilitating illnesses, Wimmer and his collaborators weren’t able to attract a pharmaceutical company willing to invest in a new technology that, he estimates, will take millions of dollars to figure out its value.“Nobody with a lot of money may want to take the risk, so we overcame that barrier right now,” he said.
Eckard Wimmer in his lab. Photo by Naif Mohammed Almojarthi
Codagenix has $6.2 million in funding. The National Institutes of Health initially contributed $600,000. The company scored an additional $1.4 million from NIH. It also raised $4.2 million from venture capital, which includes $4 million from TopSpin and $100,000 from Accelerate Long Island and a similar amount from the Center for Biotechnology at Stony Brook University.
Stony Brook University recently entered an exclusive licensing agreement with Codagenix to commercialize this viral vaccine platform. Codagenix is scheduled to begin phase I trials on a vaccine for seasonal influenza this year.
The key to this technology came from a SBU collaboration that included Wimmer, Bruce Futcher in the Department of Molecular Genetics & Microbiology and Steven Skiena in the Department of Computer Science. The team figured out a way to use gene manipulation and computer algorithms to alter the genes in a virus. The change weakens the virus, giving the attack dog elements of the immune system a strong scent to seek out and destroy any real viruses in the event of exposure.
Wimmer explained that the process starts with a thorough analysis of a virus’s genes. Once scientists determine the genetic code, they can introduce hundreds or even thousands of changes in the nucleic acids that make up the sequence. A computer helps select the areas to alter, which is a rapid process and, in a computer model, can take only one afternoon. From there, the researchers conduct experiments in tissue culture cells and then move on to experiment on animals, typically mice. This can take six months, which is a short time compared to the classical way, Wimmer said.
At this point, Codagenix has a collaboration with the Universidad de Puerto Rico at the Caribbean Primate Research Center to treat dengue and Zika virus in primates. To be sure, some promising vaccines in the past have been taken off the market because of unexpected side effects or even because they have become ineffective after the virus in the vaccine undergoes mutations that return it to its pathogenic state. Wimmer believes this is unlikely because he is introducing 1,000 changes within a vaccine candidate, which is much higher than other vaccines. In 2000, for example, it was discovered that the polio vaccines involve only five to 50 mutations and that these viruses had a propensity to revert, which was rare, to the type that could cause polio.
Colleagues suggested that this technique was promising. “This approach, given that numerous mutations are involved, has the advantage of both attenuation and genetic stability of the attenuated phenotype,” Charles Rice, the Maurice R. and Corrine P. Greenberg professor in virology at Rockefeller University explained in an email.
While Wimmer is changing the genome, he is not altering the structure of the proteins the attenuated virus produces, which is exactly the same as the virus. This gives the immune system a target it can recognize and destroy that is specific to the virus. Wimmer and his associates are monitoring the effect of the vaccines on mosquitoes that carry and transmit them to humans. “It’s not that we worry about the mosquito getting sick,” he said. “We have to worry whether the mosquito can propagate this virus better than before.” Preliminary results show that this is not the case, he said.
Wimmer said there are many safety precautions the company is taking, including ensuring that the vaccine candidate is safe to administer to humans. Wimmer moved from Berlin to Saxony after his father died when Wimmer was 3. He earned an undergraduate degree in chemistry in 1956 at the University of Rockstock. When he was working on his second postdoctoral fellowship at the University of British Columbia in Vancouver, he heard a talk on viruses, which brought him into the field.
A resident of Old Field, Wimmer lives with his wife Astrid, a retired English professor at Stony Brook. The couple’s daughter Susanne lives in New Hampshire and has three children, while their son Thomas lives in Portland, Oregon, and has one child. “We’re very happy Long Islanders,” said Wimmer, who likes to be near the ocean and Manhattan.
Through a career spanning over 50 years, Wimmer has won numerous awards and distinctions. He demonstrated the chemical structure of the polio genome and worked on polio pathogenesis and human receptor for polio. He also published the first cell-free creation of a virus.
“This was an amazing result that enabled a number of important mechanistic studies on poliovirus replication,” Rice explained. Wimmer has “always been fearless and innovative, with great enthusiasm for virology and discovery.”
With this new effort, Wimmer feels he will continue in his quest to contributing to humanity.
As the New Year begins, we are still a polarized nation because of our politics and profoundly disrespectful rhetoric. Racial hatred and violence continues to increase. Concerns about the undocumented and our broken immigration system continue to instill fear and paralyzing anxiety among so many people from so many different ethnicities. Health care is becoming a nightmare, and no one seems concerned enough to challenge the insurance companies that are continuing to sentence so many people to premature death.
The heroin epidemic continues to be a national health crisis that falls on deaf ears. Treatment beds are not increasing and with the anticipated crisis in health care, there will probably be even fewer beds for those afflicted with this life-threatening addiction we call heroin.
Although the present social and political landscape across our nation is in turmoil, there is a profound awareness that we need to live and act differently; the American dream is not dead but truly alive! Hopefully our new president will spend his first hundred days healing and unifying our nation, building bridges and not walls with his message to make “America Great Again.”
For many of us, America is already great and for me that is best seen during the holiday season. This year I was amazed that in spite of all the turmoil nationally, people’s generosity toward others, especially those in need, has been extraordinary. Each day, I see firsthand the generosity of so many talented and gifted people. Local physicians, lawyers, accountants, social workers, psychiatrist, teachers and tradespeople to name a few who volunteered to help those who are trying to navigate the difficult landscape of daily living. Thanks to the generosity of so many hands and hearts, those they touch have a chance to keep their lives on track and move forward. Without this generosity, many people in need would lose their way.
For more than two decades, I’ve been privileged to share my insights and my observations in this space. Every New Year I make a couple of recommendations as the New Year begins. This year begins a whole new chapter for us as a nation! This past election was unprecedented. The future is exciting, challenging and probably a bit frightening — because our newly elected president is not predictable — like most of life!
Probably my most important recommendations are that we reclaim a civil and respectful discourse when discussing any issue; that we work harder at respecting all people no matter what their race, creed, color, sexual orientation or political perspective. Respect costs nothing but shapes everything. It serves no purpose to gossip or malign another person’s character and reputation.
We need to work harder at being less judgmental of human circumstances and situations that we don’t understand. We should never judge another by the color of his or her skin, the clothes he or she wears, the piercings or tattoos he or she displays or the lifestyle he or she embraces. If we judge less and respect more, the violence that is infecting our communities will be substantially reduced.
My final recommendation has to do with risk-taking. Too often we see things that trouble us and we keep silent. Sometimes that silence can be lethal, especially when it comes to our children’s social behaviors. We need to speak up and step out in regards to the reckless decision-making that a number of our young people are engaging: the illegal use of alcohol, prescription medication and illegal drugs. If we care about our children and their future, we must have the courage to risk our own comfort and do the right thing.
As this New Year begins, let us be more vigilant. Let us call our government to greater accountability to be more responsive to the needs of those among us who are less fortunate. The poor and the homeless are not invisible and government should not act as if they are. We are painfully reminded that we are vulnerable and not invincible. All life is sacred but only temporary. Thus, whatever we can do to make life better, we need to do it now for we may not pass this way again.
So, let us think and act more positively with a cooperative spirit in ways that will make our community better. Let us become the change we wish to see in the world (Gandhi). Remember, you can make a difference that really counts!
Fr. Pizzarelli, SMM, LCSW-R, ACSW, DCSW, is the director of Hope House Ministries in Port Jefferson.
The Smithtown Center for the Performing Arts is currently gearing up for the second show of its 15th anniversary season, the award-winning musical play “Peter and the Starcatcher,” which will open on Jan. 14. Based on the 2006 children’s novel of “Peter and the Starcatchers,” by Dave Barry and Ridley Pearson, and adapted for the stage by Rick Elice, the play, according to the SCPA’s press release, is a swashbuckling grown-up prequel to “Peter Pan.”
The show appeared on Broadway from 2012 to 2013 and won five Tony Awards including Best Play and Best Original Score (Wayne Barker). At the time, The New York Times wrote that it was “the most exhilarating Broadway storytelling in decades.”
The role of Peter Pan will be played by 25-year-old actor David Gow, a Houston, Texas, native who graduated last May from the North Carolina School of Arts with a bachelor’s of fine arts in drama. Gow, who now resides in Harlem, was most recently in “The Beast’s Beauty” at Lincoln Center, in the role of the Beast, and in an off-broadway play titled “Chokehold.” I recently spoke with the actor about his latest role as “the boy who wouldn’t grow up.”
Why did you decide to try out for this role?
Playing Peter was at the top of my list of dream roles, so I was constantly searching for auditions for it as soon as I moved to New York. Once I saw Smithtown was doing it I was all in, and I roped my friend Emma Geer, who plays the role of Molly, into doing it too!
What is the play about?
The story slowly fills in the questions people have about Peter Pan but in a very subtle way, while simultaneously adding plot lines that are so brilliantly spontaneous the audience couldn’t possibly predict them. It’s definitely an action/adventure and has really a bit of everything in it. It switches effortlessly from action, farce and drama.
What is your favorite scene?
I love the scene where Black Stache/Captain Hook and Peter meet for the first time. There’s something so iconic about how the two of them are drawn to each other despite being mortal enemies. I also love the last scene of the play, but you’ll have to come see the show to see what happens!
What is your favorite musical number?
I like “Swim On” the best — it is the closing song of Act 1.
I understand that 12 actors will be taking on the roles of over 100 characters?
The 12 actors playing 100 roles has been the biggest challenge, but also I think the most rewarding. We really have nothing but a couple of ropes, trunks and ladders. We get to create everything else ourselves, which lets the audience jump from scene to scene instantaneously. I play a few other roles quickly, like a pirate and sailor here and there.
What is it like working with the rest of the cast?
The cast could not have been more welcoming to the actors who were new (myself included). A lot of them have done shows here for years, but I felt like we all clicked pretty immediately. There’s not a weak link in the group.
What is it like working with the director, Ken Washington?
Ken is definitely a veteran director and comes very prepared to every rehearsal. Very positive and enthusiastic about the show. It’s been such a wonderful room to come into every night.
Is this a show for all ages?
I’d say more than almost any other show, this show is ABSOLUTELY for all ages. It has the excitement and humor for adults to enjoy, while also having elements perfectly geared toward children as well. Totally appropriate.
Why should people come out to see this show?
“Peter and the Starcatcher” is to “Peter Pan” as “Wicked” is to the “Wizard of Oz.” All of your previous questions about Peter Pan are answered in this show. Come find out why Peter Pan can fly, why Captain Hook only has one hand and why none of the boys are growing up. The show has everything: nonstop action and adventure; it will make you roll on the floor laughing and also provides incredibly touching moments. I actually don’t know anyone who I would not recommend this show to. It really is for everyone!
The Smithtown Center for Performing Arts, 2 E. Main St., Smithtown, will present “Peter and the Starcatcher” from Jan. 14 to Feb. 25. Tickets are $35 adults, $32 seniors and $20 for students with a valid ID. For more information or to purchase tickets, call 631-724-3700 or visit www.smithtownpac.com.

 “Swiss cheese” as we know it doesn’t really exist. It is a generic term often used in North America for any type of cheese, regardless of where it comes from, as long as it has a pale-yellow body and is literally full of holes or “eyes,” with a rubbery texture. And this holds true for both imported and “domestic” Swiss cheeses.
“Swiss cheese” as we know it doesn’t really exist. It is a generic term often used in North America for any type of cheese, regardless of where it comes from, as long as it has a pale-yellow body and is literally full of holes or “eyes,” with a rubbery texture. And this holds true for both imported and “domestic” Swiss cheeses.