A demonstration is done at King Kullen in Patchogue, showing how to use the drug take-back dropbox added through the Department of Environmental Conservation’s pilot program that started last year. File photo from Adrianne Esposito
By Desirée Keegan
New York is taking another step toward ridding our community and our homes of dangerous drugs.
The state Assembly passed the Drug Take Back Act June 20 following the Senate’s passage of the bill the night before, which will establish a statewide program to provide free, safe pharmaceutical disposal
for unused or expired medications.
Pharmaceutical manufacturers, rather than the taxpayers, will foot the entire bill for implementing the program. Chain pharmacies will be required to provide free drug take-back sites, while other authorized collectors, like independent pharmacies and local lawenforcement, will have the option to participate.
“This landmark law makes New York a national leader in addressing the opioid crisis and protecting our waters from pharmaceutical pollution,” said Adrienne Esposito, executive director of Citizens Campaign for the Environment, applauding state Sen. Kemp Hannon (R-Garden City) and Assemblywoman Aileen Gunther (D-Middletown). “[They] have stood up for clean water, public health and New York taxpayers over the special interests of the multibillion-dollar pharmaceutical industry.
This drug take-back legislation is the best in the nation and we believe it will be adopted by other states. The cost to the pharmaceutical industry will be negligible — communities that have passed similar laws estimated a cost of just a couple pennies per prescription.”
This legislation ensures all New Yorkers will have convenient access to safe drug disposal options. Making safe disposal options accessible to the public will reduce what officials described as the harmful
and antiquated practice of flushing unwanted drugs. Drugs that are flushed are polluting waters from the Great Lakes to Long Island Sound, threatening aquatic life, water quality and drinking water.
“A lack of options to safely dispose of unused drugs is contributing to the national drug abuse epidemic that is now the leading cause of injury and death in the U.S., ahead of car accidents,” said Andrew Radin, chair of the New York Product Stewardship Council and recycling director for Onondaga County Resource Recovery Agency. “Deaths from drug overdoses and chronic drug abuse in New York state have increased 71 percent between 2010 and 2015.”
More than 2,000 people in New York die annually from opioid overdose, and 70 percent of people that abuse prescription drugs get them from friends and family, according to the Citizens Campaign for the Environment.
“The Drug Take Back Act will save lives by stopping prescription drug abuse at its source,” Radin said.
A coalition of environmental, public health and product stewardship organizations praised Gov. Andrew Cuomo (D) and the state Department of Environmental Conservation for a recently released report, called “The Feasibility of Creating and Implementing a Statewide Pharmaceutical Stewardship Program in New York State,” which called for the disposal program to be funded by the pharmaceutical industry. Cuomo asked for the report when he vetoed what he called a poorly crafted disposal bill that passed the legislature last year.
“Safe drug disposal options will help save lives by getting leftover prescription drugs out of household medicine cabinets, where they are often stockpiled and abused,” Esposito said. “We now look forward to seeing the governor sign this critical bill into law.”
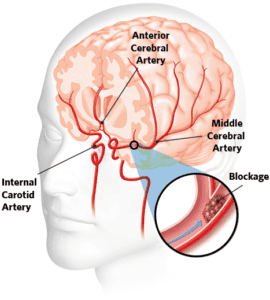
Knowing the signs of a stroke and getting help quickly can save your life.
By Ernest J. Baptiste
Ernest Baptiste
Stroke can affect people of all ages and backgrounds. When you have a stroke, you lose nearly two million brain cells for each minute that passes until normal blood flow is restored to your brain. No wonder it’s a leading cause of disability. It’s also the fifth-leading cause of death for both men and women in the United States.
We’re encouraged that there has been a decline in stroke deaths over the past few years — due in part to increased awareness of the signs of stroke, people seeking treatment faster and improvements in the types of treatments available — but our work is far from done.
Knowing the signs of stroke and getting help quickly can save your life or that of a loved one. Signs include sudden loss of balance, sudden loss of vision in one or both eyes, an uneven facial expression, numbness or weakness in one arm and/or leg or disrupted speech. If you suspect you’re having a stroke, call 911 immediately. Let the operator know and ask to be taken to a stroke center where advanced treatments are available.
It is certainly a testament to the advanced level of quality stroke care provided at Stony Brook University Hospital that our stroke center was recently certified by The Joint Commission as a Comprehensive Stroke Center — the highest level a stroke center can achieve. To receive this advanced certification, we underwent a rigorous screening process.
This certification is awarded only to institutions that provide advanced care to patients with exceptional, around-the-clock treatment.
As the first and only certified Comprehensive Stroke Center in Suffolk County — the second on Long Island and one of only 11 in New York State — Stony Brook joins an elite group. Nationally, approximately 200 hospitals out of 5,800 have earned this designation.
While we hope that you or someone you love never experiences a stroke, it’s important to know that you have the most advanced level of stroke care just minutes away at SBU. For the thousands of Long Islanders who survive a stroke and face a tough road ahead, we offer help as well.
Our Stony Brook Stroke Support Group provides encouragement and feedback from others who can relate to a stroke survivor’s and/or their family member’s situation, as well as tips about helpful programs and resources.
Although this advanced certification is a significant achievement for Stony Brook University Hospital, it is our patients and the communities we serve who benefit the most from having this level of stroke care available close to home. As a certified comprehensive stroke center, we provide a level of care that few hospitals anywhere can match.
Ernest J. Baptiste is the chief executive officer at Stony Brook University Hospital.
A heart attack does not always have obvious symptoms. Stock photo
Chest pain is only one indicator
By David Dunaief, M.D.
Dr. David Dunaief
Heart disease is the most common chronic disease in America. When we refer to heart disease, it is an umbrella term; heart attacks are one component. Fortunately, the incidence of heart attacks has decreased over the last several decades, as have deaths from heart attacks. However, there are still 720,000 heart attacks every year, and more than two-thirds are first heart attacks (1).
How can we further improve these statistics and save more lives? We can do this by increasing awareness and education about heart attacks. It is a multifaceted approach: recognizing the symptoms and knowing what to do if you think you’re having a heart attack.
If you think someone is having a heart attack, call 911 as quickly as possible and have the patient chew an adult aspirin (325 mg) or four baby aspirins. Note that the Food and Drug Administration does not recommend aspirin for primary prevention of a heart attack. However, the use of aspirin here is for treatment of a potential heart attack, not prevention. It is also very important to know the risk factors and how to potentially modify them.
Heart attack symptoms
The main symptom is chest pain, which most people don’t have trouble recognizing. However, there are a number of other, more subtle, symptoms such as discomfort or pain in the jaw, neck, back, arms and epigastric, or upper abdominal, areas. Others include nausea, shortness of breath, sweating, light-headedness and tachycardia (racing heart rate). One problem is that less than one-third of people know these other major symptoms (2). About 10 percent of patients present with atypical symptoms — without chest pain — according to one study (3).
It is not only difficult for the patient but also for the medical community, especially the emergency room, to determine who is having a heart attack. Fortunately, approximately 80 to 85 percent of chest pain sufferers are not having a heart attack. More likely, they have indigestion, reflux or other non-life-threatening ailments.
There has been a raging debate about whether men and women have different symptoms when it comes to heart attacks. Several studies speak to this topic. Let’s look at the evidence.
Men vs. women
There is data showing that, although men have heart attacks more commonly, women are more likely to die from a heart attack (4). In a Swedish prospective (forward-looking) study, after having a heart attack, a significantly greater number of women died in hospital or near-term when compared to men. The women received reperfusion therapy, artery opening treatment that consisted of medications or invasive procedures less often than the men.
However, recurrent heart attacks occurred at the same rate, regardless of sex. Both men and women had similar findings on an electrocardiogram; they both had what we call ST elevations. This was a study involving approximately 54,000 heart attack patients, with one-third of them being women.
One theory about why women are treated less aggressively when first presenting in the ER is that they have different and more subtle symptoms — even chest pain symptoms may be different. Women’s symptoms may include pain in the lower portion of the chest or upper portion of the abdomen and may have significantly less severe pain that could radiate or spread to the arms. But, is this true? Not according to several studies.
In one observational study, results showed that, though there were some subtle differences in chest pain, on the whole, when men and women presented with this main symptom, it was of a similar nature (5). There were 34 chest pain characteristic questions used to determine if a difference existed. These included location, quality or type of pain and duration. Of these, there was some small amount of divergence: The duration was shorter for a man (2 to 30 minutes), and pain subsided more for men than for women. The study included approximately 2,500 patients, all of whom had chest pain. The authors concluded that determination of heart attacks with chest pain symptoms should not factor in the sex of patients.
This trial involved an older population; patients were a median age of 70 for women and 59 for men, with more men having had a prior heart attack. This was a conspicuous weakness of an otherwise mostly solid study, since age and previous heart attack history are important factors.
Therefore, I thought it apt to present another observational study with a younger population, where there was no significant difference in age; the median age of both men and women was 49. In this GENESIS-PRAXY study, results showed that chest pain remained the most prevalent presenting symptom in both men and women (6). However, of the patients who presented without distinct chest pain and with less specific EKG findings (non-ST elevations), significantly more were women than men. Those who did not have chest pain symptoms may have had some of the following symptoms: back discomfort, weakness, discomfort or pain in the throat, neck, right arm and/or shoulder, flushing, nausea, vomiting and headache.
If the patients did not have chest pain, regardless of sex, the symptoms were, unfortunately, diffuse and nonspecific. The researchers were looking at acute coronary syndrome, which encompasses heart attacks. In this case, independent risk factors for disease not related to chest pain included both tachycardia (rapid heart rate) and being female. The authors concluded that there need to be better ways to calibrate non-chest pain symptoms.Some studies imply that as much as 35 percent of patients do not present with chest pain as their primary complaint (7).
Let’s summarize
So what have we learned about heart attack symptoms? The simplest lessons are that most patients have chest pain, and that both men and women have similar types of chest pain. However, this is where the simplicity stops and the complexity begins. The percentage of patients who present without chest pain seems to vary significantly depending on the study — ranging from less than 10 percent to 35 percent.
Therefore, it is even difficult to quantify the number of non-chest pain heart attacks. This is why it is even more important to be aware of the symptoms. Non-chest pain heart attacks have a bevy of diffuse symptoms, including obscure pain, nausea, shortness of breath and light-headedness. This is seen in both men and women, although it occurs more often in women. When it comes to heart attacks, suspicion should be based on the same symptoms for both sexes. Therefore, know the symptoms, for it may be your life or a loved one’s that depends on it.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management.
Reflux (GERD) disease, sometimes referred to as heartburn, though this is more of a symptom, is one of the most commonly treated diseases. Continuing with that theme, proton pump inhibitors (PPIs), which have become household names, are one of the top-10 drug classes prescribed or taken in the United States. In fact, Centers for Disease Control and Prevention data shows that use has grown precipitously in the 10 years ending in 2010 for those ages 55 to 64, from 9 percent of the population to 16 percent (1). This is a 78 percent increase in the number of prescriptions for these drugs.
In 2010, there were 147 million prescriptions filled for PPIs (2). The class of drugs includes Prevacid (lansoprazole), Prilosec (omeprazole), Nexium (esomeprazole), Protonix (pantoprazole) and Aciphex (rabeprazole). This growth may not capture the fact that several of these medications are now available over the counter.
I remember when PPIs were touted as having one of the cleanest side effect profiles. This may still be true, if we are using them correctly for reflux disease. They are supposed to be used for the short term. This can range from 7 to 14 days for over-the-counter PPIs to 4 to 8 weeks for prescription PPIs.
Why did we not know that this class of drugs might be associated with chronic kidney disease, dementia, bone fractures and Clostridium difficile (a bacterial infection of the gastrointestinal tract) before they were approved? Well, if you look at the manufacturers’ package inserts for these drugs, the trials, such as for Protonix, were no longer than a year (3), yet we are putting patients on these medications for decades. And the longer people are on them, the more complications arise.
Typical symptoms of reflux are heartburn and/or regurgitation. Atypical symptoms include coughing and throat clearing. But these atypical symptoms may not be as common as you might think. In fact, in one study, coughing and throat clearing taken together only resulted in a very small portion of patients having reflux disease (4). Having one of these two symptoms showed a slightly higher risk of reflux, but very modest.
Let’s look at some of the research.
Though PPIs may increase the risk of a number of complications, keep in mind that none of the data are from randomized controlled trials (RCTs), which are the gold standard of studies, but mostly observational studies that suggest an association, but not a link. Long-term RCTs to determine side effects are prohibitively expensive.
PPI and kidney disease
Recent research has tied proton pump inhibitors to a host of alarming health problems. Stock photo
In two separate studies, results showed that there was an increase in chronic kidney disease with prolonged PPI use (5). All of the patients started the study with normal kidney function based on glomerular filtration rate (GFR). In the Atherosclerosis Risk in Communities (ARIC) study, there was a 50 percent increased risk of chronic kidney disease, while the Geisinger Health System cohort study found there was a modest 17 percent increased risk. The first study had a 13-year duration, and the second had about a six-year duration. Both demonstrated a modest, but statistically significant, increased risk of chronic kidney disease.
But as you can see, the medications were used on a chronic basis for years. In an accompanying editorial to these published studies, the author suggests that there is overuse of the medications or that they are used beyond the resolution of symptoms and suggests starting with diet and lifestyle modifications as well as a milder drug class, H2 blockers (6).
PPI and bone fractures
In a meta-analysis (a group of 18 observational studies), results showed that PPIs can increase the risk of hip fractures, spine fractures and any-site fractures (8). Interestingly, when it came to bone fractures, it did not make a difference whether patients were taking PPIs for more or less than a year. How much less than a year was not delineated. They found increased fracture risks of 58, 26 and 33 percent for spine, hip and any site, respectively. It is not clear what may potentially increase the risk; however, it has been proposed that it may have to do with calcium absorption through the gut.
PPIs reduce the amount of acid, which may be needed to absorb insoluble calcium salts. In another study, seven days of PPIs were shown to lower the absorption of calcium carbonate supplements when taken without food (9).
PPI and dementia
Stock photo
A German study looked at health records from a large public insurer and found there was a 44 percent increased risk of dementia in the elderly who were using PPIs, compared to those who were not (7). These patients were at least age 75. The authors surmise that PPIs may cross the coveted blood-brain barrier and have effects by potentially increasing beta-amyloid levels, markers for dementia. With occasional use, meaning once every 18 months for a few weeks to a few months, there was a much lower increased risk of 16 percent.
The researchers also suggested that PPIs may be significantly overprescribed in the elderly. Unfortunately, there were confounding factors that may have conflated the risk, such as multiple drug use, having diabetes, or patient also having depression or a stroke history. Researchers also did not take into account family history of dementia, high blood pressure or excessive alcohol use, all of which have effects on dementia occurrence.
Need for magnesium
PPIs may have lower absorption effects on several electrolytes including magnesium, calcium and B12. In one observational study, PPIs combined with diuretics caused a 73 percent increased risk of hospitalization due to low magnesium (10). Diuretics are water pills that are commonly used in disorders such as high blood pressure, heart failure and swelling.
Another study confirmed these results. In this second study, which was a meta-analysis (a group of nine studies), PPIs increased the risk of low magnesium in patients by 43 percent, and when researchers looked only at higher quality studies, the risk increased to 63 percent (11). The authors note that a significant reduction in magnesium could lead to cardiovascular events.
The bottom line is even though some PPIs are over-the-counter and some are prescription medications, it is best if you confer with your doctor before starting them. You may not need PPIs, but rather a milder medication referred to as H2 blockers (Zantac, Pepcid). Even better, start with lifestyle modifications including diet, not eating later at night, raising the head of the bed, losing weight and stopping smoking, if needed, and then consider medications (12). If you do need medications, know that PPIs don’t give immediate relief and should only be taken for a short duration: 7 to 14 days, according to the FDA (13), without a doctor’s consult, and 4 to 8 weeks with one. Most of the problems occur with long-term use.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
Visit the Port Jefferson Free Library table at the 2018 Green Fest
Seeking to promote an eco-friendly environment and a “greener” lifestyle, the Greater Port Jefferson Chamber of Commerce will sponsor its 10th annual Green Fest on Saturday, June 16 from 1 to 5 p.m.
The free event will once again be held at the Port Jefferson Village Center at 101 East Broadway — a most fitting venue as the community hub is the result of a recycling/renovation of the historic Bayles Shipyard Building — and will feature green market vendors throughout the first floor and outside if the weather is nice.
The annual festival began a decade ago with the goal to educate, inform, entertain and enlighten people on how to make smart choices for a greener world including being energy conscious as a way to reduce our carbon footprint.
Quality Shredding will be at the event.
This year’s highlight will be a community shredding event from 1 to 3:30 p.m. by Quality Shredding of Deer Park. “We wanted to make more of an impact and add another dimension to the event,” said Barbara Ransome, director of operations at the chamber. Residents and visitors can bring up to three bags or boxes of personal papers per person to be shredded for free. The mobile truck is capable of shredding up to 10,000 pounds of personal paper.
Entertainment will include a yoga class by Satya Yoga & Pilates Studio in Mount Sinai (mats will be provided), two spiritual drumming circles with shamanic drummer Peter Maniscalco and a performance by improvisational solo street guitarist Jeff Bellanca of Classic Jam1.
Children will enjoy visiting the Port Jefferson Free Library’s Green Teens table to make a craft using recycled materials and the Sweetbriar Nature Center’s table to see their resident critters. And if your stomach starts rumbling during the event, visit the Sweet Melissa 1932 Farm to Table food truck, specializing in organic nutritional cuisine.
SERVPRO of Port Jefferson will return to the festival this year.
Of course, no festival is complete without a diverse group of over 20 select vendors highlighting green products and services including renewable solar energy, electric/hybrid and smart cars, electric bikes with live demonstrations along with a mini-farmers market offering candles, flowers, plants, soaps, yarn and baked goods for sale.
With so much going on, this family-friendly event is a great way to kick off the summer. Come on down and enjoy the day learning about methods that promote sustainable ways of living that will benefit our environment and planet and make our community a healthier place to live. The first 100 attendees will receive a free canvas bag, courtesy of SERVPRO of Port Jefferson. Making a difference begins with one small step (or fest) at a time.
Co-sponsored by Times Beacon Record News Media, Maggio Environmental Services and SERVPRO of Port Jefferson, the event will be held rain or shine. For more information, call 631-473-1414 or visit www.portjeffgreenfest.com.
Being a couch potato is detrimental to your health. Stock photo
Hint — it’s not only about weight
By David Dunaief, M.D.
Dr. David Dunaief
What causes Type 2 diabetes? It would seem like an obvious answer: obesity, right? Well, obesity is a contributing factor but not necessarily the only factor. This is important because the prevalence of diabetes is at epidemic levels in the United States, and it continues to grow. The latest statistics show that about 12.2 percent of the U.S. population aged 18 or older has Type 2 diabetes, and about 9.4 percent when factoring all ages (1).
Not only may obesity play a role, but sugar by itself, sedentary lifestyle and visceral (abdominal) fat may also contribute to the pandemic. These factors may not be mutually exclusive, of course.
We need to differentiate among sugars because form is important. Sugar and fruit are not the same with respect to their effects on diabetes, as the research will help clarify. Sugar, processed foods and sugary drinks, such as fruit juices and soda, have a similar effect, but fresh fruit does not.
Sugar’s impact
Sugar may be sweet, but it also may be a bitter pill to swallow when it comes to its effect on the prevalence of diabetes. In an epidemiological (population-based) study, the results show that sugar may increase the prevalence of Type 2 diabetes by 1.1 percent worldwide (2). This seems like a small percentage; however, we are talking about the overall prevalence, which is around 9.4 percent in the U.S., as we noted above.
Also, the amount of sugar needed to create this result is surprisingly low. It takes about 150 calories, or one 12-ounce can of soda per day, to potentially cause this rise in diabetes. This is looking at sugar on its own merit, irrespective of obesity, lack of physical activity or overconsumption of calories. The longer people were consuming sugary foods, the higher the incidence of diabetes. So the relationship was a dose-dependent curve.
Interestingly, the opposite was true as well: As sugar was less available in some countries, the risk of diabetes diminished to almost the same extent that it increased in countries where it was overconsumed.
In fact, the study highlights that certain countries, such as France, Romania and the Philippines, are struggling with the diabetes pandemic, even though they don’t have significant obesity issues. The study evaluated demographics from 175 countries, looking at 10 years’ worth of data. This may give more bite to municipal efforts to limit the availability of sugary drinks. Even steps like these may not be enough, though. Before we can draw definitive conclusion from the study, however, there need to be prospective (forward-looking) studies.
The effect of fruit
The prevailing thought has been that fruit should only be consumed in very modest amounts in patients with — or at risk for — Type 2 diabetes. A new study challenges this theory. In a randomized controlled trial, newly diagnosed diabetes patients who were given either more than two pieces of fresh fruit or fewer than two pieces had the same improvement in glucose (sugar) levels (3). Yes, you read this correctly: There was a benefit, regardless of whether the participants ate more fruit or less fruit.
This was a small trial with 63 patients over a 12-week period. The average patient was 58 and obese, with a body mass index of 32 (less than 25 is normal). The researchers monitored hemoglobin A1C (HbA1C), which provides a three-month mean percentage of sugar levels. It is very important to emphasize that fruit juice and dried fruit were avoided. Both groups also lost a significant amount of weight while eating fruit. The authors, therefore, recommended that fresh fruit not be restricted in diabetes patients.
What about cinnamon?
It turns out that cinnamon, a spice many people love, may help to prevent, improve and reduce sugars in diabetes. In a review article, the authors discuss the importance of cinnamon as an insulin sensitizer (making the body more responsive to insulin) in animal models that have Type 2 diabetes (4).
Cinnamon may work much the same way as some medications used to treat Type 2 diabetes, such as GLP-1 (glucagon-like peptide-1) agonists. The drugs that raise GLP-1 levels are also known as incretin mimetics and include injectable drugs such as Byetta (exenatide) and Victoza (liraglutide). In a study with healthy volunteers, cinnamon raised the level of GLP-1 (5). Also, in a randomized control trial with 100 participants, 1 gram of cassia cinnamon reduced sugars significantly more than medication alone (6). The data is far too preliminary to make any comparison with FDA-approved medications. However it would not hurt, and may even be beneficial, to consume cinnamon on a regular basis.
Sedentary lifestyle
What impact does lying down or sitting have on diabetes? Here, the risks of a sedentary lifestyle may outweigh the benefits of even vigorous exercise. In fact, in a recent study, the authors emphasize that the two are not mutually exclusive in that people, especially those at high risk for the disease, should be active throughout the day as well as exercise (7).
So in other words, the couch is “the worst deep-fried food,” as I once heard it said, but sitting at your desk all day and lying down also have negative effects. This coincides with articles I’ve written on exercise and weight loss, where I noted that people who moderately exercise and also move around much of the day are likely to lose the greatest amount of weight.
Thus, diabetes is most likely a disease caused by a multitude of factors, including obesity, sedentary lifestyle and visceral fat. The good news is that many of these factors are modifiable. Cinnamon and fruit seem to be two factors that help decrease this risk, as does exercise, of course.
As a medical community, it is imperative that we reduce the trend of increasing prevalence by educating the population, but the onus is also on the community at large to make at least some lifestyle modifications. So America, take an active role.
References:
(1) www.cdc.gov/diabetes. (2) PLoS One. 2013;8(2):e57873. (3) Nutr J. published online March 5, 2013. (4) Am J Lifestyle Med. 2013;7(1):23-26. (5) Am J Clin Nutr. 2007;85:1552–1556. (6) J Am Board Fam Med. 2009;22:507–512. (7) Diabetologia online March 1, 2013.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
Some seemingly innocent activities can increase risk
By David Dunaief, M.D.
Dr. David Dunaief
Warmer weather is finally upon us, and we now have long, sunny days. However, longer sun exposure does increase the risk of skin cancer. Melanoma is the most serious skin cancer, but fortunately it is not the most common. Basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (SCC) are more prevalent, in that order. Here, we will focus on these two types.
The incidences of these skin cancers are very difficult to pin down because they are not always reported. However, most of us either know someone who has had these types of skin cancer or have had them ourselves. There were roughly three million people diagnosed with nonmelanoma skin cancer in the U.S. in 2012, with the number of treatments increasing 77 percent from 1994 to 2014 (1). SCC and BCC outcomes diverge, with the former having a higher risk of metastases compared to the latter, which tends to grow much slower (2).
These skin cancers may present in different ways. BCC may have a bump that is pearly, waxy, light-colored or pink or flesh-colored or brown. It may bleed, ooze and crust, but may not heal, and can be sunken in the middle (3). SCC has the appearance of a growing nodule. It may also be scaly or crusty and may have flat reddish patches. It may be a sore that also may not heal. It is found on sun-exposed areas, more commonly the forehead, hands, lower lip and nose (3). Interestingly, SCC develops over years of gradual ultraviolet sun exposure, while BCC develops more like melanoma through intense multiple sporadic burns (4).
The more well-known risks for these types of skin cancer include sun exposure (UV radiation), light skin, age, ethnicity and tanning beds (2). But there are other risk factors, such as manicures. There are also ways to reduce risk with sunscreen reapplied every two hours, depending on what you are doing, but also NSAIDs (nonsteroidal anti-inflammatory drugs) and even vitamin B3. Let’s look at the research.
Ultraviolet radiation from the sun or tanning beds can cause skin cancer. Stock photo
Risks of other cancers
Though nonmelanoma skin cancers (NMSCs) have far less potential to be deadly, compared to melanoma, there are other risks associated with them. In the CLUE II cohort study of over 19,000 participants, results show something very disturbing: A personal history of NMSC can lead to other types of cancer throughout the body (5). The increased risk of another type of cancer beyond NMSC is 103 percent in those with BCC and 97 percent in those with SCC, both compared to those who did not have a personal history of NMSC.
Tanning beds — No surprise
We know that tanning beds may be a cause for concern. Now the FDA has changed the classification of tanning beds from low to moderate risk and requires a warning that they should not be used by those under the age of 18 (6). Some states have more restrictive laws, banning tanning bed use or requiring parental consent when teens are below certain ages. Compliance with these laws varies.
However, in a prospective (forward-looking) study, results show that people’s responses to warnings depended on how the warnings were framed (7). Compared to the text-only FDA warning requirement, graphic warnings that emphasized the risks of skin cancer were more likely to help people stop using tanning beds, whereas graphic warnings that demonstrated the positive benefits of not using these devices had no effects. So you may have to scare the daylights out of those in their teens and early twenties.
Manicure risk, really?
I am told women and some men love manicures. Manicures cannot possibly be dangerous, right? Not so fast. It is not the actual manicure itself, but rather the drying process that poses a risk. In a prospective study, results show that drying lamps used after a manicure may increase the risk of DNA damage to the skin, which could lead to skin cancer, though the risk is small per visit (8).
There were a lot of variables. The shortest number of visits to increase the risk of skin cancer was eight, but the intensity of the UVA irradiance varied considerably in 17 different salons. The median number of months it took to have carcinogenic potential with exposure was around 35, or roughly three years. The authors recommend either gloves or suntan lotion when using these devices, although both seem to be somewhat impractical with wet nails. It’s best to let your nails dry naturally.
Vitamin B3 to the rescue
Many vitamins tend to disappoint when it comes to prevention. Well, hold on to your hat. This may not be the case for vitamin B3. In the Australian ONTRAC study, the results showed that vitamin B3 reduced the risk of developing NMSC by 23 percent, compared to those who took a placebo (9). Even better was the fact that SCC was reduced by 30 percent.
The most interesting part about this study is that these results were in high-risk individuals who had a personal history of NMSC. The participants were given B3 (nicotinamide 500 mg) twice daily for one year.
After the patients discontinued taking B3, the benefits dissipated within six months. The study was on the small side, including 386 patients with two or more skin cancer lesions in the last five years, with a mean of eight lesions. The side effects were minimal and did not include the flushing (usually neck and facial redness) or headaches seen with higher levels of niacin, another derivative. The caveat is that this study was done in Australia, which has more intense sunlight. We need to repeat the study in the U.S. Nicotinamide is not expensive, and it has few side effects.
NSAIDs as beneficial?
Results have been mixed previously in terms of NSAIDs and skin cancer prevention. However, a more recent meta-analysis (nine studies of varying quality, with six studies considered higher quality) showed that especially nonaspirin NSAIDs reduced the risk of SCC by 15 percent compared to those who did not use them (10).
Diet — The good and the bad
In terms of diet studies, there have been mixed positive and neutral results, especially when it comes to low-fat diets. These are notoriously difficult to run because the low-fat group rarely remains low fat. However, in a prospective dietary study, results showed that effects on skin cancer varied depending on the foods. For those who were in the highest tertile of meat and fat consumption, compared to those in the lowest tertile, there was a threefold increased risk of a squamous cell cancer in those who had a personal history of SCC (11). But what is even more interesting is that those who were in the highest tertile of vegetable consumption, especially green leafy vegetables, experienced a 54 percent reduction in skin cancer, compared to those in the lowest consumption tertile.
Thus, know that there are modifiable risk factors that reduce the risk of nonmelanoma skin cancer and don’t negatively impact your enjoyment of summer. There may be easy solutions to help prevent recurrent skin cancer, as well, that involve both medication and lifestyle modifications.
References:
(1) skincancer.org. (2) uptodate.com. (3) nih.gov. (4) Br J Cancer. 2006;94(5):743. (5) J Natl Cancer Inst. 2008;100(17):1215-1222. (6) federalregister.gov. (7) Am J Public Health. Online June 11, 2015. (8) JAMA Dermatol. 2014;150(7):775-776. (9) ASCO 2015 Annual Meeting: Abstract 9000. (10) J Invest Dermatol. 2015;135(4):975-983. (11) Am J Clin Nutr. 2007;85(5):1401.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
TIAs are a serious warning sign of stroke and should not be ignored.
Ministrokes are not inconsequential
By David Dunaief, M.D.
Dr. David Dunaief
A TIA (transient ischemic attack) is sometimes referred to as a ministroke. This is a disservice since it makes a TIA sound like something that should be taken lightly. Ischemia is reduced or blocked blood flow to the tissue, due to a clot or narrowing of the arteries. Symptoms may last less than five minutes. However, a TIA is a warning shot across the bow that needs to be taken very seriously on its own merit. It may portend life-threatening or debilitating complications that can be prevented with a combination of medications and lifestyle modifications.
Is TIA common?
It is diagnosed in anywhere from 200,000 to 500,000 Americans each year (1). The operative word is “diagnosed,” because it is considered to be significantly underdiagnosed. I have helped manage patients with symptoms as understated as the onset of double vision. Other symptoms may include facial or limb weakness on one side, slurred speech or problems comprehending others, dizziness or difficulty balancing or blindness in one or both eyes (2). TIA incidence increases with age (3).
What is a TIA?
TIAs are a serious warning sign of stroke and should not be ignored.
The definition has changed over time from one purely based on time (less than one hour), to differentiate it from a stroke, to one that is tissue based. It is a brief episode of neurological dysfunction caused by focal brain ischemia or retinal ischemia (low blood flow in the back of the eye) without evidence of acute infarction (tissue death) (4). In other words, TIA has a rapid onset with potential to cause temporary muscle weakness, creating difficulty in activities such as walking, speaking and swallowing, as well as dizziness and double vision.
Why take a TIA seriously if its debilitating effects are temporary?
Though they are temporary, TIAs have potential complications, from increased risk of stroke to heightened depressive risk to even death. Despite the seriousness of TIAs, patients or caregivers often delay receiving treatment.
Stroke risk
After a TIA, stroke risk goes up dramatically. Even within the first 24 hours, stroke risk can be 5 percent (5). According to one study, the incidence of stroke is 11 percent after seven days, which means that almost one in 10 people will experience a stroke after a TIA (6). Even worse, over the long term, the probability that a patient will experience a stroke reaches approximately 30 percent, one in three, after five years (7).
To go even further, there was a study that looked at the immediacy of treatment. The EXPRESS study, a population-based study that considered the effect of urgent treatment of TIA and minor stroke on recurrent stroke, evaluated 1,287 patients, comparing their initial treatment times after experiencing a TIA or minor stroke and their subsequent outcomes (8).
The Phase 1 cohort was assessed within a median of three days of symptoms and received a first prescription within 20 days. In Phase 2, median delays for assessment and first prescription were less than one day. All patients were followed for two years after treatment. Phase 2 patients had significantly improved outcomes over the Phase 1 patients. Ninety-day stroke risk was reduced from 10 to 2 percent, an 80 percent improvement.
The study’s authors advocate for the creation of TIA clinics that are equipped to diagnose and treat TIA patients to increase the likelihood of early evaluation and treatment and decrease the likelihood of a stroke within 90 days. The moral of the story is: Treat a TIA as a stroke should be treated, the faster the diagnosis and treatment, the lower the likelihood of sequela, or complications.
Predicting the risk of stroke complications
Both DWI (diffusion weighted imaging) and ABCD2 are potentially valuable predictors of stroke after TIA. The ABCD2 is a clinical tool used by physicians. ABCD2 stands for Age, Blood pressure, Clinical features and Diabetes, and it uses a scoring system from 0 to 7 to predict the risk of a stroke within the first two days of a TIA (9).
Heart attack
In one epidemiological study, the incidence of a heart attack after a TIA increased by 200 percent (10). These were patients without known heart disease. Interestingly, the risk of heart attacks was much higher in those over 60 years of age and continued for years after the event. Just because you may not have had a heart attack within three months after a TIA, this is an insidious effect; the average time frame for patients was five years from TIA to heart attack. Even patients taking statins to lower cholesterol were at higher risk of heart attack after a TIA.
Mortality
If stroke and heart attack were not enough, TIAs decrease overall survival by 4 percent after one year, by 13 percent after five years and by 20 percent after nine years, especially in those over age 65, according to a study published in Stroke (11). The reason younger patients had a better survival rate, the authors surmise, is that their comorbidity (additional diseases) profile was more favorable.
Depression
In a cohort (particular group of patients) study that involved over 5,000 participants, TIA was associated with an almost 2.5-times increased risk of depressive disorder (12). Those who had multiple TIAs had a higher likelihood of depressive disorder. Unlike with stroke, in TIA it takes much longer to diagnose depression, about three years after the event.
What can you do?
Awareness and education are important. While 67 percent of stroke patients receive education about their condition, only 35 percent of TIA patients do (13). Many risk factors are potentially modifiable, with high blood pressure being at the top of the list, as well as high cholesterol, increasing age (over 55) and diabetes.
Secondary prevention (preventing recurrence) and prevention of complications are similar to those of stroke protocols. Medications may include aspirin, antiplatelets and anticoagulants. Lifestyle modifications include a Mediterranean and DASH diet combination. Patients should not start an aspirin regimen for chronic preventive use without the guidance of a physician.
In researching information for this article, I realized that there are not many separate studies for TIA; they are usually clumped with stroke studies. This underscores the seriousness of this malady. If you or someone you know has TIA symptoms, the patient needs to see a neurologist and a primary care physician and/or a cardiologist immediately for assessment and treatment to reduce risk of stroke and other long-term effects.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
Linda Nuszen, Maryann Natale and Janet D'Agostino, parents who have lost children to opioid addiction, during an event dedicating a new garden at St. Charles Hospital May 18. Photo by Kyle Barr
They say it’s becoming impossible to walk through a crowd and not find at least one person who hasn’t been affected by the opioid crisis. On May 18 a group of more than 50 people, nearly all of whom have lost loved ones, or at least experienced the strain of a loved one having gone through the throws of addiction, gathered at St. Charles Hospital for the unveiling of a new “Remembrance and Reflection Garden” just outside the Infant Jesus Chapel on hospital grounds.
The idea started with Port Jefferson resident Marcia Saddlemire, whose daughter Nicole passed away as a result of opioid addiction in 2015. She said she didn’t want to leave the memory of her daughter as just an opioid addict.
“I was getting angry watching the news, when they say so many died from overdose in Suffolk County this year, I said dammit, she’s not a statistic, she’s a person, she has a name and a life,” Saddlemire said. “All the mothers agree with this, they don’t want to grow up to be addicts. This is not what they wanted from their lives, they had dreams, they had goals.”
Stones dedicated to families affected by opioid addiction in a new garden at St. Charles Hospital. Photo by Kyle Barr
Saddlemire said she didn’t have the connections or know-how to create such a project, so she managed to get in contact with three women — Janet D’Agostino, Maryann Natale and Linda Nuszen — all of whom belong to multiple anti-opioid organizations and support groups. They gathered together to plan and create the new garden.
“We want it to be public — we don’t want to hide it,” said Natale, whose son Anthony died of an overdose. “We want them to know it’s an epidemic. This garden also helps those families who are going through such time with an addict.”
St. Charles Hospital was chosen as the location for the garden because of its existing programs fighting opioid addiction, according to the mothers. The hospital has 40 beds that are allotted for chemical dependency rehabilitation, 10 for supervised detoxification for adults and four for detoxification of adolescents age 12 to 18. Jim O’Connor, the executive vice president of St. Charles Hospital, said administration expects to receive another 10 beds for detoxification services. He said he also expects to develop an outpatient center at the hospital for addicts who need ongoing, comprehensive care in the next several years.
“We are honored that these families have chosen St. Charles Hospital as the site for this very special garden, as St. Charles is committed to hosting hospital programs which combat Suffolk County’s current addiction crisis,” O’Connor said.
Stones dedicated to families who have lost loved ones to opioid addiction in a new garden at St. Charles Hospital. Photo by Kyle Barr
Nearly all work for the project was donated by local businesses. The garden includes stones engraved with the names of victims of opioid addiction and quotes from their families. Ron Dennison and his son Alan from Bohemia-based Long Island Water Jet donated their time to create a heart sign featured in the garden. The sign features large words like “forgiveness” and “understanding” along with small words like “pain” and “fear,” to show positive emotions overcoming the negative.
Dennison’s daughter, Sarah, went through the St. Charles rehab program when she became addicted to opioids. She is out of the program now, and she has a daughter named Serenity.
“When your kids are addicted, you deny it, you deny it, you deny it,” the elder Dennison said as he fought to speak through tears. “And then one day you wake up you say, ‘what is going on here.”
Nuszen and her family founded Look Up for Adam, a foundation dedicated to her son who died from an overdose in 2015. Her organization helps to raise awareness.
“So many people don’t know how to show up for our loved ones,” she said. “So many people don’t know how to be themselves, or how to be here for each other. So now that we can come here and have a place where we’re not isolated — so they come here and know they’re not alone, that there are people who care about them.”
It is very important to take white-coat hypertension seriously. Stock photo
As many as 30 percent of patients experience this phenomenon
By David Dunaief, M.D.
Dr. David Dunaief
White-coat hypertension (high blood pressure) is defined as blood pressure that is elevated to at least 140/90 mm Hg at a physician’s office, but “normal” when measured at home. The blood pressure considered normal at home for most Americans is less than 135/85 mm Hg. This is a real phenomenon caused by the anxiety or stress of being in a doctor’s office. It is also known as “isolated office hypertension.”
About 15 to 30 percent of patients experience white-coat hypertension (1). However, when the diastolic (bottom number) blood pressure is greater than 105 mm Hg, it is unlikely to be simply caused by doctor’s office-related stress (2).
Consequences
What are the consequences of white-coat hypertension? The first challenge is that physicians may overtreat it, prescribing medications that lead to low blood pressure when not in the office. Alternately, we sometimes discount it because it seems benign or harmless. However, some studies show that it may increase the risk of sustained hypertension, which is a major contributor to developing cardiovascular disease — heart disease and stroke.
It is very important to take white-coat hypertension seriously because Centers for Disease Control and Prevention data show that the percentage of adults age 20 and over with hypertension reached 33.5 percent in the 2013-14 period (3).
What can be done?
What can be done about white-coat hypertension? Well, it does not need to be treated with medication, except potentially in elderly patients (over 80 years of age) but should involve lifestyle modifications, including dietary changes, stress reduction and exercise. In terms of diet, increased beet juice, green leafy vegetables and potassium, as well as decreased sodium intake may be important. You should monitor the blood pressure at home, taking multiple readings during the day, or by 24-hour ambulatory blood pressure readings, which require wearing a monitor. The latter provides the additional advantage of blood pressure readings during your sleep.
If you do monitor your blood pressure at home, the American Heart Association has suggestions on how to get the most accurate readings, such as measurements early in the morning before exercising and eating, as well as in the evening (4). You should also be comfortably seated, don’t cross your legs, and sit/relax for a few minutes before taking a reading. Let’s look at the evidence.
Risk of sustained high blood pressure
There were no substantial studies demonstrating any consequences from white-coat hypertension until 2005. Most previous studies on white-coat hypertension were not of long enough duration.
In the 2005 population-based Ohasama study, results showed that the participants who had white-coat hypertension were 2.9 times more likely to develop sustained hypertension, compared to those who had normal blood pressure in the doctor’s office (5). There were almost 800 participants involved in this study, with a mean age at the start of 56. What was really impressive about the study was its duration, with an eight-year follow-up. This gives a better sense of whether white-coat hypertension may develop into sustained hypertension. The researchers concluded that it may lead to a less than stellar outlook for cardiovascular prognosis.
Another study, published in 2009, reinforced these results. The PAMELA study showed that those with white-coat hypertension had about a 2.5-times increased risk of developing sustained high blood pressure, compared to those who had normal readings in all environments (6). There were 1,412 participants involved in the study, ranging in age from 25 to 74. Just like the previous study, an impressive aspect was the fact that there was a long follow-up period of 10 years. Thus, this was a substantial study, applicable to the general population over a significant duration.
Prevention of sustainedhypertension
In a small, randomized controlled trial, beet juice was shown to reduce blood pressure significantly (7). Patients either were given 250 ml (about 8 ounces) of beet juice or comparable amounts of water. The patients who drank the beet juice saw an 11.2 mm Hg decrease in blood pressure, while those who drank water saw a 0.7 mm Hg reduction. This effect with the beet juice continued to remain significant. Even after 24 hours, there was a sustainable 7.2 mm Hg drop in blood pressure, compared to readings taken prior to drinking the juice. Although these results are encouraging, we need to study whether these effects can be sustained over the long term. Also, this study was done in patients with high blood pressure. I don’t know of any prevention studies done in patients with white-coat hypertension.
The researchers believe the effect is caused by high nitrate levels in beet juice that are converted to nitrite when it comes in contact with human saliva. Nitrite helps to vasodilate, or enlarge blood vessels, and thus helps to decrease blood pressure in a similar way as some antihypertensive (blood pressure) medications. The authors go on to surmise that green leafy vegetables offer protection from cardiovascular disease in part due to increased nitrite levels, similar to those in beet juice.
A subsequent double-blind, placebo-controlled clinical trial with 68 hypertensive patients found that blood pressure was significantly reduced in the clinic and in home readings over a four-week period, when compared to nitrate-free beet juice (8).
If you have diabetes, prediabetes, a family history or a high risk for diabetes, I recommend eating beets instead, since drinking beet juice will raise your sugar levels.
Increasing potassium levels significantly through food sources, not supplements, has a profound effect in reducing blood pressure. In a study where 3,500 to 4,700 mg of potassium were consumed through foods, the systolic (top number) blood pressure was reduced by 7.1 mm Hg (9). We should be getting 4,700 mg of potassium daily, which equates to about 10 bananas daily. Almonds, raisins and green leafy vegetables, such as Swiss chard, also have significant amounts of potassium.
White-coat hypertension should not be neglected. It is important to monitor blood pressure at home for at least three days with multiple readings, and then send them to your physician for review. Though patients don’t need to be on blood pressure medications at this stage, it does not mean you should be passive about the process. Make lifestyle modifications to reduce your risk of developing sustained hypertension.
References:
(1) Hypertension. 2013;62:982-987, originally published Nov 13, 2013. (2) J Hypertens. 2001;19(6):1015. (3) cdc.gov. (4) Am Fam Physician. 2005 Oct 1;72(7):1391-1398. (5) Arch Intern Med. 2005 Jul 11;165(13):1541-1546. (6) Hypertension. 2009; 54: 226-232. (7) Hypertension. Online 2013; April 15. (8) Hypertension. 2015 Feb; 65(2): 320–327. (9) BMJ. 2013 Apr 3;346:f1378.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.