CURIOUS ORIOLE Stony Brook resident Jay Gao captured this image of a Baltimore oriole in his backyard garden over the summer using a Nikon D5500. This songbird has most likely already migrated to its wintering grounds, which include Florida, the Caribbean, Central America and the northern tip of South America.
Lentils may not be the most attractive foods when cooked, but they do pack a powerful nutritional and delicious wallop. Low in fat and high in protein and fiber, they are a staple of many Asian cuisines.
When I looked them up in my old cookbooks, they often were absent. However, in my newer and more recent cookbooks, they occupy a whole column in the indexes, a gift of the many immigrants and ethnicities that have become a part of our American culture.
I would venture to say that lentils are one of the go-to elements for ethnic as well as vegetarian recipes and are an ideal addition to anyone’s pantry for a quick-cooking, tasty and nourishing dish that welcomes and complements other flavors. From the familiar greenish-tan ones to tiny green Puy lentils to red (actually salmon pink) lentils, with many other varieties along the spectrum, their mild earthy flavor has captured many a palate.
Lentil Salad with Tomatoes and Herbs
Lentil Salad with Tomatoes and Herbs
YIELD: Makes 4 servings
INGREDIENTS:
1 cup green Puy or black beluga lentils, rinsed
2 teaspoons salt
1 large garlic clove, minced
12 ounces fresh tomatoes, chopped
²/3 cup thinly sliced scallions
1 handful fresh dill, chopped
¼ cup extra virgin olive oil
2 tablespoons red wine vinegar
Salt and freshly ground black pepper, to taste
DIRECTIONS: Fill a large saucepan with one quart cold water; add lentils, garlic and two teaspoons salt and bring to a boil. Reduce heat and simmer, uncovered, until lentils are just tender, about 20 minutes. Drain and transfer to a large bowl. Toss hot lentils with tomatoes, scallions, dill, oil and vinegar. Season with salt and pepper to taste. Serve hot or warm with lamb or chicken and tossed green salad.
Lentil Soup
Lentil Soup
YIELD: Makes 8 to 10 servings
INGREDIENTS:
2 cups lentils
9 cups cold water
Salt and freshly ground pepper, to taste
1 large onion, chopped
2 ribs celery, sliced thin
2 carrots, peeled and diced
1 tablespoon fresh thyme leaves or 1 teaspoon dried
1 bay leaf
½ teaspoon sugar
2 to 3 tablespoons wine vinegar
Juice of one lemon
DIRECTIONS: Place lentils in a large pot and cover with the 9 cups water; add salt and pepper, onion, celery, carrot, thyme, bay leaf and sugar. Bring to a boil and simmer 45 minutes or until lentils are tender. Remove bay leaf and discard. Scoop out 2 to 3 cups of the lentil and vegetable mixture and puree in a food processor. Return puree to remaining soup, stir and bring back to a boil. Stir in vinegar, a tablespoon at a time, until just a hint of its flavor is evident. Serve hot with cucumber salad and hearty bread.
Red Lentil Curry
Red Lentil Curry
YIELD: Makes 4 servings
INGREDIENTS:
¼ cup vegetable oil
2 tablespoons minced fresh ginger
2 cloves garlic, minced
1 bunch scallions, trimmed and sliced
1 tablespoon plus 1 teaspoon curry powder
2 cups diced carrots
1 sweet potato, peeled and diced
1 cup red lentils
4 cups vegetable or chicken broth
Salt and pepper, to taste
1 handful fresh chives, chopped or sliced
DIRECTIONS: In a large saucepan heat the oil over medium-high heat. Add ginger, garlic and scallions and cook, stirring frequently, until softened, about 2 to 3 minutes. Stir in the curry powder, carrots, sweet potato, lentils, broth and salt and pepper. Stir, bring to a boil, then simmer until lentils and veggies are tender, about 15 to 20 minutes. Sprinkle with chives. Serve hot with naan bread and rice.
Arthritis, a history of stroke and Parkinson’s disease can contribute to fall risk.
Increased risk can begin at the age of 45
By David Dunaief, M.D.
Dr. David Dunaief
When we are young, falls usually do not result in significant consequences. However, when we reach middle age and chronic diseases become more prevalent, falls become more substantial. And, unfortunately, falls are a serious concern for older patients, where consequences can be devastating. They can include brain injuries, hip fractures, a decrease in functional ability and a decline in physical and social activities (1). Ultimately, falls can lead to loss of independence (2).
Of those over the age of 65, between 30 and 40 percent will fall annually (3). Most of the injuries that involve emergency room visits are due to falls in this older demographic (4).
What can increase the risk of falls?
Many factors contribute to fall risk. A personal history of falling in the recent past is the most prevalent. But there are many other significant factors, such as age; being female; and using drugs, like antihypertensive medications used to treat high blood pressure and psychotropic medications used to treat anxiety, depression and insomnia.
Chronic diseases, including arthritis, as an umbrella term; a history of stroke; cognitive impairment and Parkinson’s disease can also contribute. Circumstances that predispose us to falls also involve weakness in upper and lower body strength, decreased vision, hearing disorders and psychological issues, such as anxiety and depression (5).
How do we prevent falls?
Fortunately, there are ways to modify many risk factors and ultimately reduce the risk of falls. Of the utmost importance is exercise. But what do we mean by “exercise”? Exercises involving balance, strength, movement, flexibility and endurance, whether home based or in groups, all play significant roles in fall prevention (6). We will go into more detail below.
Many of us in the Northeast suffer from low vitamin D, which may strengthen muscle and bone. This is an easy fix with supplementation. Footwear also needs to be addressed. Nonslip shoes, if recent winters are any indication, are of the utmost concern. Inexpensive changes in the home, like securing area rugs, can also make a big difference.
Medications that exacerbate fall risk
There are a number of medications that may heighten fall risk. As I mentioned, psychotropic drugs top the list. Ironically, they also top the list of the best-selling drugs. But what other drugs might have an impact?
High blood pressure medications have been investigated. A propensity-matched sample study (a notch below a randomized control trial in terms of quality) showed an increase in fall risk in those who were taking high blood pressure medication (7). Surprisingly, those who were on moderate doses of blood pressure medication had the greatest risk of serious injuries from falls, a 40 percent increase. One would have expected those on the highest levels to have the greatest increase in risk, but this was not the case.
While blood pressure medications may contribute to fall risk, they have significant benefits in reducing the risks of cardiovascular disease and events. Thus, we need to weigh the risk-benefit ratio, specifically in older patients, before considering stopping a medication. When it comes to treating high blood pressure, lifestyle modifications may also play a significant role in treating this disease (8).
Where does arthritis fit into this paradigm?
In those with arthritis, compared to those without, there is an approximately two-times increased risk of two or more falls and, additionally, a two-times increased risk of injury resulting from falls, according to the Centers for Disease Control and Prevention (1). This survey encompassed a significantly large demographic; arthritis was an umbrella term including those with osteoarthritis, rheumatoid arthritis, gout, lupus and fibromyalgia.
Therefore, the number of participants with arthritis was 40 percent. Of these, about 13 percent had one fall and, interestingly, 13 percent experienced two or more falls in the previous year. Unfortunately, almost 10 percent of the participants sustained an injury from a fall. Patients 45 and older were as likely to fall as those 65 and older.
Why is exercise critical?
All exercise has value. A meta-analysis of a group of 17 trials showed that exercise significantly reduced the risk of a fall (9). If the categories are broken down, exercise had a 37 percent reduction in falls that resulted in injury and a 30 percent reduction in those falls requiring medical attention. Even more impressive was a 61 percent reduction in fracture risk.
Remember, the lower the fracture risk, the more likely you are to remain physically independent. Thus, the author summarized that exercise not only helps to prevent falls but also fall injuries. The weakness of this study was that there was no consistency in design of the trials included in the meta-analysis. Nonetheless, the results were impressive.
Unfortunately, those who have fallen before, even without injury, often develop a fear that causes them to limit their activities. This leads to a dangerous cycle of reduced balance and increased gait disorders, ultimately resulting in an increased risk of falling (10).
What specific types of exercise are useful?
Many times, exercise is presented as a word that defines itself. In other words: Just do any exercise and you will get results. But some exercises may be more valuable or have more research behind them. Tai chi, yoga and aquatic exercise have been shown to have benefits in preventing falls and injuries from falls.
A randomized controlled trial, the gold standard of studies, showed that those who did an aquatic exercise program had a significant improvement in the risk of falls (11). The aim of the aquatic exercise was to improve balance, strength and mobility. Results showed a reduction in the number of falls from a mean of 2.00 to a fraction of this level — a mean of 0.29. There was no change in the control group.
There was also a 44 percent decline in the number of patients who fell. This study’s duration was six months and involved 108 postmenopausal women with an average age of 58. This is a group that is more susceptible to bone and muscle weakness. Both groups were given equal amounts of vitamin D and calcium supplements. The good news is that many patients really like aquatic exercise.
Thus, our best line of defense against fall risk is prevention. Does this mean stopping medications? Not necessarily. But for those 65 and older, or for those who have “arthritis” and are at least 45 years old, it may mean reviewing your medication list with your doctor. Before considering changing your BP medications, review the risk-to-benefit ratio with your physician. The most productive way to prevent falls is through lifestyle modifications.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
Many boomers plan on using their assets to make their golden years golden.
By Linda M. toga, Esq.
Linda M. Toga, Esq.
THE FACTS: My husband and I are in our sixties and have three grown children. All were given the same opportunities growing up, but they did not all take advantage of those opportunities or make wise decisions about their futures. Our two daughters are financially secure and doing very well. Our son, however, has struggled and we expect will continue to struggle to make ends meet his entire life.
My husband and I have accumulated significant assets over the years. We have been generous to our children and have made an effort to treat them all the same despite the differences in their financial well-being.
Despite this fact, my son seems to be under the impression that because he needs more, he is entitled to more. He has made comments on a number of occasions suggesting that since we have the means to make his life easier, we should do so. It is clear that he expects that we will be leaving him a sizable inheritance, perhaps even more than we leave our daughters.
We are bothered by these comments for a number of reasons, not the least of which is that my husband and I are planning on using our hard earned money to travel and, if needed, to cover our health care costs. While we fully expect that all of our children will inherit some money from us, I do not believe that we will be leaving any of them substantial assets.
THE QUESTION: How do we make this clear to our son who seems to think he will see a windfall when we die?
THE ANSWER: You and your husband are not alone in having accumulated significant assets that you hope to spend on yourselves. Many boomers benefited by parents who were conservative savers and cautious spenders. Consequently, these parents often accumulated more wealth than they spent and passed that wealth on to their boomer children.
The boomers, on the other hand, may not have been such conscientious savers. Even if they were, they are finding that they are living longer, may need more money for health care and often believe that they need not leave substantial assets to their children since they did so much for them during their lives.
Like you and your husband, many boomers plan on using their assets to make their golden years golden. That is your right. You earned it. You can spend it. However, if you do not want your son to be surprised or resentful when he does not inherit the kind of money he may expect will be coming his way, the best thing to do is to tell him outright.
Perhaps you can share with him the choices you made over the years that resulted in having a significant nest egg. Then tell him how you hope to spend your hard earned money on yourselves while you enjoy a long and healthy life.
You may discover that the comments he has made about a large inheritance were made in jest and that he isn’t really counting on a windfall. That would be the best scenario.
Even if he expresses disappointment and/or anger, you and your husband should feel better about the fact that you were open and honest with him. He can ignore what you say or he can use what you tell him to better plan for his future. In either case, having the conversation will ensure that when you and your husband pass away, he is not blindsided.
Linda M. Toga provides personalized service and peace of mind to her clients in the areas of elder law, estate administration and estate planning, real estate, marital agreements and litigation. Visit her website at www.lmtogalaw.com or call 631-444-5605 to schedule a free consultation.
MEET BLUE! This sweet and energetic puppy is Blue. An 8-month-old male husky mix, he just recently came from Puerto Rico to Kent Animal Shelter and he is looking for a loving home with a big backyard to run and play for the rest of his days. One look into his blue and brown eyes and you will be hooked! Blue comes neutered, microchipped and up to date on all his vaccines. Kent Animal Shelter is located at 2259 River Road in Calverton. For more information on Blue and other adoptable pets at Kent, please call 631-727-5731 or visit www.kentanimalshelter.com.
Update: Blue is still available for adoption as of Dec. 21.
Long Island is an ideal environment for many species of ticks, specifically the deer tick.
By Matthew Kearns, DVM
I commonly get the question, “What month can I stop using tick preventatives?” My answer is always, “That depends.” It used to be that somewhere around late October/November until late March/early April one could stop using flea and tick preventatives. However, with changing climate conditions and parasite adaptation this is no longer true.
The tick life cycle contains four stages: egg, larval, nymph (young adult) and adult. After the larval stage hatches out from the egg, it must feed and go through a molt between each successive stage. Ticks are sensitive to environmental changes throughout their life cycle but, ironically, are most resistant to temperature changes. It has to be below 35°F for ticks to even “overwinter.”
Overwinter is a term that refers to a process many species use to pass through the period of the year when “winter” conditions (cold or sub-zero temperatures, ice, snow, limited food supplies) make normal activity or even survival difficult or near impossible. During the overwinter period all activity nearly completely ceases until conditions become more favorable. If conditions become more favorable (above 45°F) ticks will set out in search of a host.
To kill a tick temperatures must be consistently below 10°F for many days in a row. If the tick is able to bury itself in the vegetation below a layer of snow, even below 10 degrees may not kill them. It is pretty routine even in January to have one or two days that are in the 20s during the day, dropping to the teens or single digits at night followed by a few days in the 50s.
Ironically, as resistant as ticks are to colder temperatures, they are much more sensitive to higher temperatures and humidity (or lack thereof). Eggs will desiccate, or dry out, and die during hot dry periods. The other life stages are at risk for dehydration due to increased respiratory rate in an effort to thermoregulate (control body temperature) and questing (looking for hosts).
Hotter, drier temperatures mean less vegetation. Less vegetation causes multiple problems for ticks: less protection from the elements and less vegetation for hosts.
The white-footed mouse is the primary host for the larval stage of the deer tick. This mouse survives on vegetation, and less vegetation and less resources for the mouse means a subsequent decrease in the mouse population. A decrease in population means less hosts. Less hosts, less ticks survive from the larval stage to adulthood. Fortunately, and unfortunately for us, the northeast United States rarely sees prolonged droughts. Even if we have hot, dry periods during the summer, we usually make up for it in the fall. It is an ideal environment for many species of ticks, specifically the deer tick.
In summary, it is my feeling that the tick season is 9 to 10 months out of the year. You may be able to stop applying preventative during the months of January, February, and March (this depends on temperature), but the rest of the year ticks are active.
Dr. Kearns practices veterinary medicine from his Port Jefferson office and is pictured with his son Matthew and his dog Jasmine.
One of the marvels of being a conscious organism is our capacity to interpret the things we do.
By Elof Axel Carlson
Elof Axel Carlson
Nedra had her right knee replaced on Sept. 13, 2017, and our daughter Christina and I waited in Indiana University’s General Hospital in Bloomington. She was groggy after some of the anesthesia wore off, and I was surprised that during the same day she was shown how to get out of bed and use a walker to get to the bathroom.
The next day she learned from an occupational therapist how to dress and undress. Also that second day she learned about 10 different exercises in bed to move her right leg. This included sliding her foot along the bed back and forth with her knee elevated and doing a half snow angel movement with her right leg.
I vaguely knew that the mechanics of body motion were first worked out by Giovanni Borelli (1608-1679). Borelli was taught by one of Galileo’s students and was skilled in mathematics, physics and medicine. He also used a microscope for his studies and discovered the stomata of plant leaves and the corpuscles in blood. He did experiments and claimed all body motion is caused by muscle contractions and he worked out the mathematics of animal motion, identifying where the limbs were in relation to the body’s center of gravity.
One of the marvels of being a conscious organism is our capacity to interpret the things we do. Many of those things — like walking, running, holding things or grooming our bodies — we do without a knowledge of the science that is involved in making them possible. We also assign other functions to body motions besides their pragmatic uses. Nedra and I both take Tai Chi for Arthritis at our local YMCA and the slow graceful motions provide exercise of all our joints. The “chi,” or vital energy, I equate in my mind with the same sensation as phantom limbs for amputees, which is neurologically based and not a psychiatric lament for the slow withdrawal of that feeling.
Body motion is paramount for those who dance, relating motion to music and the bonding and unbonding of partners as they go through a dance routine. Judo and tae kwan do are martial arts and can be used for aggressive or defensive activities among combatants. Yoga provides a spiritual aspect to body motion accompanied by meditation for those who practice it. Virtually all of us enjoy spectator sports whether watching baseball, football, basketball, tennis or the myriad of activities in winter or summer Olympic Games.
Anatomists today are well acquainted with the way muscles and bones and their tendons interact for any motion of our limbs, neck, head, hands, feet or other parts of our body. The one activity I did not include in this list is one that I find particularly appealing. The name given to it was by Thoreau who tells us in his Walden diaries that he enjoyed sauntering. It is walking with no direction or goal in mind, just wandering about in the woods or along a stream to take in the delights of nature and to stimulate thoughts for his writing.
When I was in high school and as an undergraduate, I loved solitary walks through Central Park in Manhattan, and my favorite discovery was a spot where I could sit and there were no buildings from Central Park West or Fifth Avenue visible to my eye. I thought of myself as an urban nature boy.
Nedra spent three days in the hospital and she then moved to a rehabilitation facility in a retirement community called Bell Trace. It is nice to see Nedra doing her exercises, converting pain into progress, and we look forward to her returning to our home which will be safety checked before she arrives to prevent slips and falls. For those coming days and weeks our daughter Erica, followed by two of our granddaughters and their husbands, will be out to enjoy Nedra’s progress to experience the confident walking by those with successful knee surgery enjoy.
Elof Axel Carlson is a distinguished teaching professor emeritus in the Department of Biochemistry and Cell Biology at Stony Brook University.
Insomnia is frustrating because it does not necessarily have one cause.
Untreated insomnia can have long-term health effects
By David Dunaief, M.D.
Dr. David Dunaief
Insomnia is an all-too-common complaint. Though the statistics vary widely, about 30 percent of Americans are affected, according to the most frequently used estimate, and women tend to be affected more than men (1). Insomnia is thought to have several main components: difficulty falling asleep, difficulty staying asleep, waking up before a full night’s sleep and sleep that is not restorative or restful (2).
Unlike sleep deprivation, patients have plenty of time for sleep. Having one or all of these components is considered insomnia. There is debate about whether or not it is actually a disease, though it certainly has a significant impact on patients’ functioning (3).
Insomnia is frustrating because it does not necessarily have one cause. Causes can include aging; stress; psychiatric disorders; disease states, such as obstructive sleep apnea and thyroid dysfunction; asthma; medication; and it may even be idiopathic (of unknown cause). It can occur on an acute (short term), intermittent or chronic basis. Regardless of the cause, it may have a significant impact on quality of life. Insomnia also may cause comorbidities (diseases), two of which we will investigate further: heart failure and prostate cancer.
Fortunately, there are numerous treatments. These can involve medications, such as benzodiazepines like Ativan and Xanax. The downside of these medications is they may be habit forming. Nonbenzodiazepine hypnotics (therapies) include sleep medications, such as Lunesta (eszopiclone) and Ambien (zolpidem). All of these medications have side effects. We will investigate Ambien further because of its warnings.
There are also natural treatments, involving supplements, cognitive behavioral therapy and lifestyle changes.
Let’s look at the evidence.
Heart failure
Insomnia may perpetuate heart failure, which can be a difficult disease to treat. In the HUNT analysis (Nord-Trøndelag Health Study), an observational study, results showed insomnia patients had a dose-dependent response for increased risk of developing heart failure (4). In other words, the more components of insomnia involved, the higher the risk of developing heart disease.
There were three components: difficulty falling asleep, difficulty maintaining sleep and nonrestorative sleep that is not restful. If one component was involved, there was no increased risk. If two components were involved, there was a 35 percent increased risk, although this is not statistically significant.
However, if all three components were involved, there was a 350 percent increased risk of developing heart failure, even after adjusting for other factors. This was a large study, involving 54,000 Norwegians, with a long duration of 11 years.
Prostate cancer
Prostate cancer has a plethora of possible causes, and insomnia may be a contributor. Having either of two components of insomnia, difficulty falling asleep or staying asleep (sleep disruption), increased the risk of prostate cancer by 1.7 and 2.1 times, respectively, according to an observational study (5).
However, when looking at a subset of data related to advanced or lethal prostate cancer, both components, difficulty falling asleep and sleep disruption, independently increased the risk even further, 2.1 and 3.2 times, respectively.
This suggests that sleep is a powerful factor in prostate cancer, and other studies have shown that it may have an impact on other cancers as well. There were 2,102 men involved in the study with a duration of five years. While there are potentially strong associations, this and other studies have been mostly observational. Further studies are required before any definitive conclusions can be made.
What about potential treatments?
Ambien: While nonbenzodiazepine hypnotics may be beneficial, this may come at a price. In a report by the Drug Abuse Warning Network, part of the Substance Abuse and Mental Health Services Administration (SAMHSA), the number of reported adverse events with Ambien that perpetuated emergency department visits increased by more than twofold over a five-year period from 2005 to 2010 (6). Insomnia patients most susceptible to having significant side effects are women and the elderly. The director of SAMHSA recommends focusing on lifestyle changes for treating insomnia: by making sure the bedroom is sufficiently dark, getting frequent exercise and avoiding caffeine.
In reaction to this data, the FDA required the manufacturer of Ambien to reduce the dose recommended for women by 50 percent (7). Ironically, sleep medication like Ambien may cause drowsiness the next day — the FDA has warned that it is not safe to drive after taking extended-release versions (CR) of these medications the night before.
Magnesium: The elderly population tends to suffer the most from insomnia, as well as nutrient deficiencies. In a double-blinded, randomized controlled trial (RCT), the gold standard of studies, results show that magnesium had resoundingly positive effects on elderly patients suffering from insomnia (8).
Compared to a placebo group, participants given 500 mg of magnesium daily for eight weeks had significant improvements in sleep quality, sleep duration and time to fall asleep, as well as improvement in the body’s levels of melatonin, a hormone that helps control the circadian rhythm.
The strength of the study is that it is an RCT; however, it was small, involving 46 patients over a relatively short duration.
Cognitive behavioral therapy
In a study, just one 2½-hour session of cognitive behavioral therapy delivered to a group of 20 patients suffering from chronic insomnia saw subjective, yet dramatic, improvements in sleep duration from 5 to 6½ hours and decreases in sleep latency from 51 to 22 minutes (9). The patients who were taking medication to treat insomnia experienced a 33 percent reduction in their required medication frequency per week. The topics covered in the session included relaxation techniques, sleep hygiene, sleep restriction, sleep positions and beliefs and obsessions pertaining to sleep. These results are encouraging.
It is important to emphasize the need for sufficient and good-quality sleep to help prevent, as well as not contribute to, chronic diseases, such as cardiovascular disease and prostate cancer. While medications may be necessary in some circumstances, they should be used with the lowest possible dose for the shortest amount of time and with caution, reviewing possible drug-drug and drug-supplement interactions.
Supplementation with magnesium may be a valuable step toward improving insomnia. Lifestyle changes including sleep hygiene and exercise should be sought, regardless of whether or not medications are used.
References: (1) Sleep. 2009;32(8):1027. (2) American Academy of Sleep Medicine, 2nd edition, 2005. (3) Arch Intern Med. 1998;158(10):1099. (4) Eur Heart J. online 2013;Mar 5. (5) Cancer Epidemiol Biomarkers Prev; 2013;22(5):872–879. (6) SAMSHA.gov. (7) FDA.gov. (8) J Res Med Sci. 2012 Dec;17(12):1161-1169. (9) APSS 27th Annual Meeting 2013; Abstract 0555.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.
The white petals of Large-Cupped N. 'Roulette' are a perfect foil for the orange and yellow frilled corona.
By Kyrnan Harvey
No need to panic, there’s plenty of time to order bulbs. True, some varieties might be sold out, but the importers ship through December and bulbs can be planted as long as the ground isn’t frozen. I have, in the past, gotten away with planting after New Year’s.
Above, fragrant Narcissus ‘Kedron’ (jonquilla class) naturalized with other daffodils and myrtle
I once had a garden with soil on the sandy side, enriched in the early years with wood-chip mulch, which eventually decomposes into humus. Here many kinds of tulips were naturalized. They need good drainage, and no excessive irrigation, in the summer months when they are dormant, or else they will rot. If I had planted five of one variety in 1998, by 2008 bulbs had increased with offsets that were flowering size. Tulips growing informally through forget-me-nots and among many other spring flowers and shrubs — as opposed to a stiffly formal throwaway mass display planting — are incomparably charming. But they are said to be caviar to deer.
Daffodils though are 100 percent deer proof. Nor do squirrels dig for them as they do for tulips. I like to plant them in a similar style: many different varieties, each segregated from other varieties. I don’t like daffodil “mixes” — five or 10 bulbs, spaced a few inches apart, randomly arranged (meaning asymmetrically, nongeometrically). In two or three years these bulbs will have a dozen or more flowers. Daffodils increase and naturalize far more reliably than tulips.
There are many more varieties of Narcissus than will be seen at Home Depot or a garden center. Thirty years ago, when I was employed as a gardener at Mrs. Whitney’s Manhasset estate, we participated in a flower show at Macy’s Herald Square. The head gardener, my boss, presented an instructional display with examples from each of the 13 divisions of daffodils, as established by the Royal Horticultural Society: trumpets, large-cupped and small-cupped N. triandrus, N. jonquilla, N. poeticus and so on.
Above, the charming Narcissus jonquilla ‘Kokopelli’
You can find, via numerous stateside bulb importers (Brent & Becky’s, John Scheepers, White Flower Farm), splendid cultivars from any and all of these classes. Moreover, within each division, there are many variations of form and diversity of color: white perianth (the petals) with yellow or orange or pink corona (the cup, or trumpet); yellow perianth/orange cup; white perianth/white cup. The rims of the cups can have different colors too and the cups and petals can have various forms.
It is easy to fill your garden with many different long-lived daffodils, each of which has its own distinctive charm and all of which, when viewed collectively in the vernal garden, harmonize with their compadres. You can do better than merely more ‘Mount Hood’ and ‘King Alfred.’ Many are delightfully scented, which is not, by the way, the cloying odor of the florists’ tender paperwhite narcissus. If you plant a dozen varieties this year, in five years you will be able to fill vases with bountiful, perfumed bouquets.
Daffodils tolerate full sun and part shade. The pink-cupped ones prefer the latter because it preserves their color. Deep shade and water-logged soil must be avoided. Cut the spent flowers but the leaves must be left uncut, unbent, and unbraided for weeks after flowering is finished. Finding companion perennials that disguise this unsightly phase of the growth cycle — and that won’t be chowed by deer! — is a finer aspect of horticulture best left to another day.
Kyrnan Harvey is a horticulturist and garden designer residing in East Setauket. For more information, visit www.boskygarden.com.
Mark Twain, that delightful old curmudgeon, called cauliflower “a cabbage with a college education,” a proclamation that today would probably be found politically incorrect in some way by someone. I prefer to call cauliflower a vegetable with autumn in its soul — especially here on Long Island where cauliflower farms still exist out on the East End. For me, no autumn is officially ushered in until I have made a pilgrimage to the North Fork, until I have bought too many enormous heads of cauliflower for a couple of dollars a piece at most from some roadside flatbed truck.
Heading home with the late afternoon sun slanting against the windshield, there will also be baskets and sacks of late season tomatoes, cucumbers, apples, Brussels sprouts and peppers, of Seckel pears and cider and gourds and weird shaped pumpkins all wedged into the car’s trunk.
But it will be the cauliflowers I covet most as I watch the russet leaves drift roadward. It will be the cauliflower I single out for that night’s dinner as I stuff the refrigerator’s vegetable drawers with my afternoon’s harvest. For dinner there will very likely be a pasta with cauliflower and sausage. Another night there will be a savory cauliflower salad or hearty cauliflower mashed potatoes. The following weekend I will get out my canning equipment and put up jars of chow-chow with many more little cauliflower florets than the recipe calls for. And my husband, who is also a big cauliflower fan, will nevertheless be relieved that my annual cauliflower fest is over.
Pasta with Cauliflower and Sausage
Pasta with Cauliflower and Sausage
YIELD: Makes 4 to 6 servings
INGREDIENTS:
1 pound pasta, preferably ziti or shells
3 sweet Italian sausages
1 medium cauliflower broken into small florets
½ cup extra virgin olive oil
1½ pounds fresh Italian plum tomatoes, coarsely chopped
4 garlic cloves, minced
1 tablespoon fresh thyme leaves or 1 teaspoon dried
Salt and crushed red pepper flakes, to taste
¾ cup freshly grated pecorino or romano cheese
DIRECTIONS: Bring a large pot of salted water to a boil for the pasta and cook according to package directions. Meanwhile in a medium skillet, cook the sausages over medium heat until browned on all sides; remove and set aside to keep warm. When they are cool enough to handle, cut them into bite-size pieces. Steam the cauliflower until it is al dente (slightly resistant to the bite), about 3 to 5 minutes. Set aside.
In same skillet used to cook sausages, heat half the olive oil over medium heat: add tomatoes, half the garlic and the thyme. Season and cook, stirring occasionally, over medium heat until most of the liquid is evaporated. In another medium skillet, heat the remaining oil, add the remaining garlic and steamed cauliflower and sauté until cauliflower is slightly golden. Add the sliced sausages to the cauliflower and continue cooking until sausages are reheated.
Pour cooked pasta into a large bowl, top with tomato mixture, then sausages and cauliflower. Adjust seasoning, then sprinkle with grated cheese. Mix at the table and serve with fried peppers, crusty bread and a crunchy green salad.
Cauliflower Mashed Potatoes
Cauliflower Mashed Potatoes
YIELD: Makes 8 servings
INGREDIENTS:
1 medium head cauliflower, in pieces
6 potatoes, pared and coarsely chopped
½ stick butter
¹/3 cup milk or cream
2 eggs
Salt and freshly ground pepper, to taste
¼ cup golden raisins
¼ cup pignoli nuts
DIRECTIONS: Steam the cauliflower and potatoes until they are very soft, about 20 minutes. Preheat oven to 400 F. Grease a large soufflé dish or casserole. Mash cauliflower and potatoes by hand to break up pieces. Transfer to large bowl of electric mixer. Add butter, milk or cream, eggs and salt and pepper. Beat slowly at first, then increase mixer speed gradually until mixture is smooth. Stir in raisins. Transfer to prepared casserole dish. Sprinkle top with pignoli nuts. Bake until mixture is hot and pignoli nuts are golden, about 30 to 40 minutes. Serve with meat or poultry and a mixed salad. This is a revision of an article written by the author and published in this newspaper in 1989.
Cauliflower Salad
YIELD: Makes 6 servings
INGREDIENTS:
1 medium head cauliflower, broken into bite-size florets
1 tablespoon capers, rinsed and drained
4 flat anchovy fillets, minced
½ cup oil-cured black olives
¼ pound feta cheese, diced
¹/3 cup extra-virgin olive oil
2 to 3 tablespoons wine vinegar
Coarse salt and freshly ground black pepper, to taste
1 medium red onion, thinly sliced, separated into rings, then chopped
1 cup cherry tomatoes, halved
1 tablespoon fresh dill, chopped
DIRECTIONS: Steam the cauliflower until just tender, about 5 minutes; let cool to room temperature. In a small bowl combine the capers, anchovies, olives and feta cheese with the oil, vinegar, salt and pepper. Combine with cauliflower. Cover and let the cauliflower marinate at room temperature at least an hour. Just before serving, add the onion, tomatoes and dill. Serve with meat or poultry, pasta or eggplant.











 MEET BLUE! This sweet and energetic puppy is Blue. An 8-month-old male husky mix, he just recently came from Puerto Rico to Kent Animal Shelter and he is looking for a loving home with a big backyard to run and play for the rest of his days. One look into his blue and brown eyes and you will be hooked! Blue comes neutered, microchipped and up to date on all his vaccines. Kent Animal Shelter is located at 2259 River Road in Calverton. For more information on Blue and other adoptable pets at Kent, please call 631-727-5731 or visit www.kentanimalshelter.com.
MEET BLUE! This sweet and energetic puppy is Blue. An 8-month-old male husky mix, he just recently came from Puerto Rico to Kent Animal Shelter and he is looking for a loving home with a big backyard to run and play for the rest of his days. One look into his blue and brown eyes and you will be hooked! Blue comes neutered, microchipped and up to date on all his vaccines. Kent Animal Shelter is located at 2259 River Road in Calverton. For more information on Blue and other adoptable pets at Kent, please call 631-727-5731 or visit www.kentanimalshelter.com.
 I commonly get the question, “What month can I stop using tick preventatives?” My answer is always, “That depends.” It used to be that somewhere around late October/November until late March/early April one could stop using flea and tick preventatives. However, with changing climate conditions and parasite adaptation this is no longer true.
I commonly get the question, “What month can I stop using tick preventatives?” My answer is always, “That depends.” It used to be that somewhere around late October/November until late March/early April one could stop using flea and tick preventatives. However, with changing climate conditions and parasite adaptation this is no longer true.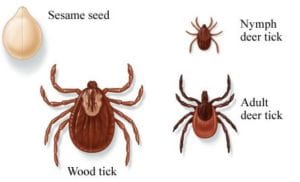 To kill a tick temperatures must be consistently below 10°F for many days in a row. If the tick is able to bury itself in the vegetation below a layer of snow, even below 10 degrees may not kill them. It is pretty routine even in January to have one or two days that are in the 20s during the day, dropping to the teens or single digits at night followed by a few days in the 50s.
To kill a tick temperatures must be consistently below 10°F for many days in a row. If the tick is able to bury itself in the vegetation below a layer of snow, even below 10 degrees may not kill them. It is pretty routine even in January to have one or two days that are in the 20s during the day, dropping to the teens or single digits at night followed by a few days in the 50s.











