Lit luminaires light up the night during the third annual Lights of Hope event in Port Jefferson on Aug. 31. Photo by Nora Milligan
It’s no time to pass the buck.
When it comes to the rising opioid abuse issue coursing through Long Island’s veins, we want to make sure we continue the open dialogue.
As you finish reading this edition, we hope you reflect on how this growing problem affects you, your family, your friends and everyone else around you — we can’t hide from this.
We need to take a more head-on approach to this medical issue, and accept that it is a medical problem, and not as some say a moral failing.
Parents shouldn’t let the stigma attached to drug or substance abuse keep them from talking about it. If we are to learn and grow and recover, we need to be talking. If we hide from the issue, the results will most certainly be fatal.
This is a problem that requires a collaborative effort, including prevention through education and early identification of at-risk people, enforcement with sharper penalties to dealers and prescription writers and improved rehabilitation resources and strategies. And as this issue should reflect, many groups on the North Shore are dedicated to working together to fight this crisis.
A cooperative combination of all of these things can help get Long Island headed in the right direction. Listed below are several resources if you or a loved one is struggling with substance or drug abuse.
• Suffolk County Substance Abuse Hotline: 631-979-1700
• Hope House Ministries: 631-978-0188
• Response of Suffolk County 24-hour hotline: 631-751-7500
• Prevention Resource Center: 631-650-0135
• Phoenix House’s Edward D. Miller substance abuse treatment center: 844-296-9046
• St. Charles Hospital rehab program: 631-474-6233
• New York State HOPEline: 1-877-8-HOPENY
• Suffolk County Division of Community Mental Hygiene Services: 631-853-8500
Visit https://www.suffolkcountyny.gov/substanceabuse for a downloadable prevention, treatment and recovery services directory, which gives a list of service agencies and treatment centers on Long Island.
This week’s issues of Times Beacon Record Newspapers are set up a little differently.
Suffolk County has one of the highest rates of death from heroin and opioid overdoses in New York State, and we feel this growing drug abuse problem deserves a special journalistic spotlight. So we dedicated this issue to looking at the different angles of approaching the heroin and opioid problem. In this week’s paper, you will find facts: How much the substance abuse trend has grown throughout the past few years; how our local communities, governments, police departments and residents have adapted to fight back against this movement; and reflections from recovering addicts and parents who have lost children to drug overdoses.
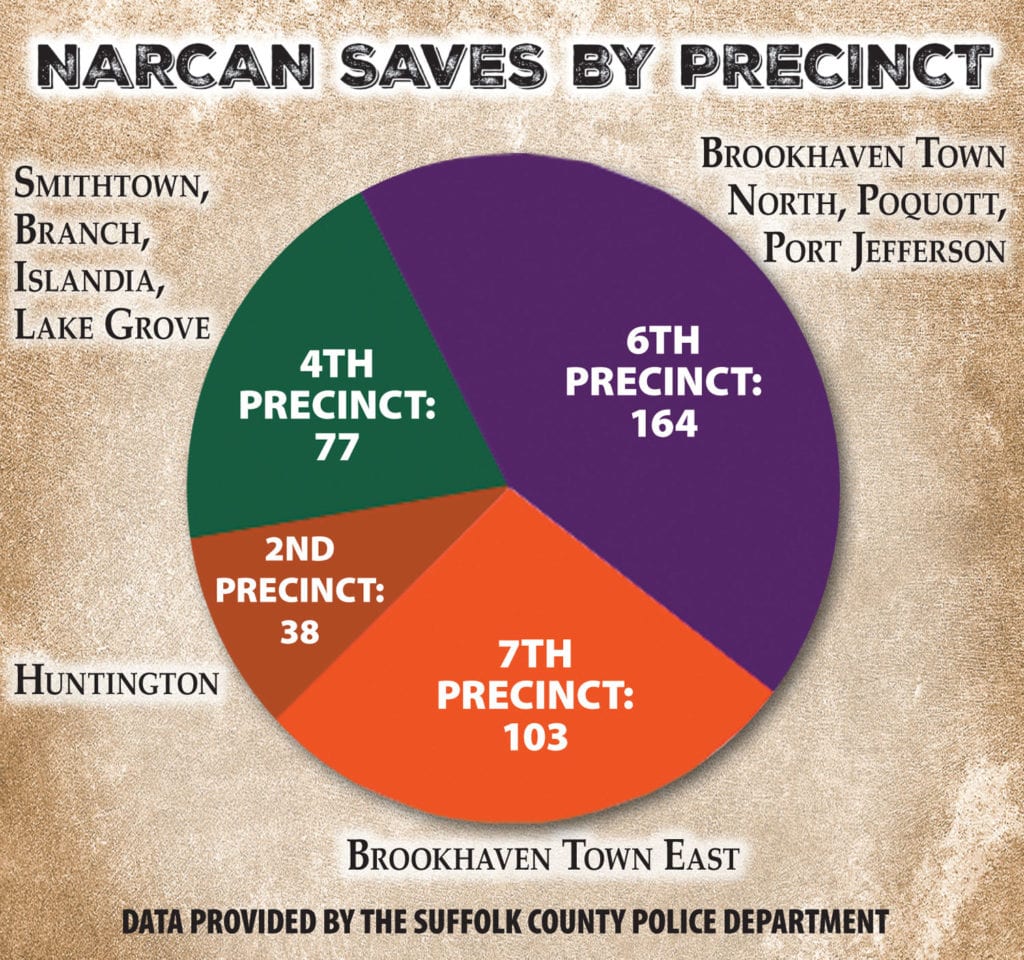
The Suffolk County Police Department has saved more than 600 lives since 2012 using Narcan to reverse opioid or heroin overdoses. Data from SCPD.Graphic by TBR News Media
Medical professionals, law enforcement and government officials gathered at Stony Brook University this past weekend to have an open and honest dialogue about the growing opioid problem facing the North Shore and the rest of Suffolk County.
The complexity of the problem and how it relates to communities across the county was the topic of the discussion Oct. 1. A common theme among the speakers was opioid addiction should be treated like a legitimate medical crisis and not a moral failing.
Dr. Constantine Ioannou, director of Stony Brook Medical Center’s Adult Inpatient Unit addressed the current opioid crisis in the United States and specifically in Suffolk County during the event.
“This is not the first opioid epidemic in the United States — this is one of many,” Ioannou said. He likened the current state of opioid prescribing and subsequent widespread addiction to a period in the late 1800s when morphine was first developed. He said doctors overprescribed the powerful painkiller and, in turn, opioid dependence skyrocketed.
SCPD Deputy Sheriff Mike Kern speaks about the opioid crisis in Suffolk County. Photo by Alex Petroski
The director traced the origin of the current crisis back to two events in 1995. Purdue Pharma, a pharmaceutical company, began marketing OxyContin, its version of the powerful opioid oxycodone, to doctors. In addition the American Pain Society, an organization dedicated to advocating for public policies to reduce pain-related issues, named pain as the fifth vital sign. Like the other four — pulse rate, temperature, respiration rate and blood pressure —pain would be monitored in patients from then on. Pain was the only one of those five vital signs that is completely subjective and based on what a patient tells a nurse or doctor, Ioannou said.
Those two events, in accordance with nurse ratings and even payment being tied to patient satisfaction and reduction, created an environment of overprescribing, Ioannou said. He also said training of doctors in pain management needs to be addressed — he graduated from medical school in 1985 with “zero” training in pain management.
“There are states in the United States where there are more prescriptions for opiate pain medications than there are people — this is a staggering number,” Ioannou said.
Jermaine Jones, Ph.D., an assistant professor of clinical neurobiology in the Department of Psychiatry at Columbia University, also spoke and reiterated some of what Ioannou said regarding the United States’ views on pain management.
“I’ve had friends from other countries say that unless you come into the E.R. with an arm missing, you’re not going to get a prescription that you could get here for having a root canal,” Jones said. “We make up about 5 percent of the world’s population yet we consume about 80 percent of the prescription opioid [painkillers].”
Jones is involved in a study called Risks and Benefits of Overdose Education and Naloxone Prescribing to Heroin Users and spoke about some of his findings. Naloxone, commonly known by the brand name Narcan, is a drug used to reverse opioid overdoses.
“We’re trying to better understand how to tease apart ways to attenuate what people like about opioids,” Jones said of the five-year study, which is currently in its second year.
Jermaine Jones, Ph.D., an assistant professor of clinical neurobiology in the Department of Psychiatry at Columbia University, was on the opioid discussion panel. Photo by Alex Petroski
He said the study was created to monitor people who are administered naloxone and see if it is being used for the correct purposes. One concern in the creation of an overdose reversal drug is that users will be more confident in their ability to combat an overdose and may decide not to call 911 if that day ever comes. Other potential unintended consequences of naloxone, including how to deal with a user who may be irate after being saved from an overdose and is now “dope sick” and without the expensive drug they just bought, are the focus of the study. They are also researching some potential new medications or existing ones that could work in accordance with opioids to reduce pain, while reducing the effects that lead to addiction.
“We know that detox by itself is actually one of the highest risk factors for opioid overdose because you’re tolerance decreases,” Jones said. “So once someone comes out of a detox program they swear they’re never going to touch this stuff again, but relapse is very, very common. So they use again thinking that if they were using two bags before, they can continue using two bags now that they’ve gotten out, but their physiological tolerance has decreased and people overdose as a result.”
Ioannou indicated he’d like to see changes in treatment options for addicts.
“We treat all addiction by the same model,” he said. “You have a five-day detox, 28-day rehab and you have an after care that is all based on 12 steps. That is the model of care in the United States. We need to realize with a complex disease, you need a complex set of interventions.”
Suffolk County Police Department Deputy Sheriff Mike Kern is an expert in recognizing drug users. He called overdoses the most powerful “advertisement” for drug dealers because it is a clear indication of how strong their product is. He echoed sentiments from both doctors about the dangers of overprescribing and to what it can lead.
“Why can a doctor prescribe an OxyContin to a 16-year-old or a 15-year-old who just had a root canal?” Kern asked. “It just doesn’t make any sense.”
In 2002, my 16-year-old son Kevin had surgery on his shoulder for a football injury. He was prescribed 60 Vicodin pills with no other instructions but to take one or two of them every four to six hours for pain.
I didn’t know they weren’t like antibiotics, and you weren’t supposed to take all 60. He was still in pain, so they gave him 60 more. Well, guess who is now addicted to them? He was buying them during lunch.
This is the high school quarterback. His girlfriend is the cheerleading captain. He is beautiful, loving, fun and funny. His friends love him. His teachers and coaches love him. He has not an enemy in the world. He graduates. He works. He is a great kid.
Kevin chose to smoke pot instead of taking the pills soon after high school, but at some point he went back to the pills — especially since I was on him all of the time to stop smoking. He had multiple concussions over his high school football career. After his last one, I saw a change in his personality. He was easily angered, depressed, anxious — all things he was not before.
I didn’t know at the time that marijuana and opioids help make all of those symptoms so much better. The drugs make them disappear. I didn’t know that the only enemy he did have was the one within himself.
Tracey Farrell and her son Kevin Norris in 2010. Photo from Tracey Farrell
When Kevin went back to the pills, he began snorting them this time. A lot of them. Once I saw a powder residue on his glass desk and, only knowing what I saw on TV, I put it on my tongue to see if it would numb it.
Nope, not cocaine.
I knew deep down something was going on. He didn’t shower as often or take care of his teeth. Changes in his habits were starting to happen.
These Oxycodone pills are expensive, and make you painfully sick when you don’t have them. An addict becomes so desperate that they will beg, borrow and steal to get them — literally. Eventually when you have exhausted stealing your family’s available cash, you steal their jewelry, sports memorabilia and anything else of value you can sneak out of the house. You write bad checks from your mom’s bank account. Eventually you realize there’s an alternative available and you turn to heroin. It’s cheap, and readily available. You just have to put money in your mailbox and drugs appear moments later.
That point happened some time in 2011. I assume he started snorting it before he shot it.
Nine years in and I am still clueless, uneducated, unaware to so much of it. Kevin never, ever looked high in front of me. I was missing spoons, which are used to melt the heroin down to a soluble form, but I still thought maybe they were thrown out by mistake? Yes, he had been to rehab, but I didn’t know that it didn’t fix you. I didn’t know that me giving him no option but to enter rehab wouldn’t work. I didn’t know that he had to want to be in recovery.
I learned how to be manipulated. I enabled everything. I believed every lie he told me and would hand over money in fear he would be killed for the money he owed.
Eventually, he must leave the house. Kevin would live in his car, on which I was now making the payments and insuring. It’s winter and I cannot fathom the thought of him in a car at Christmas, so I get him an apartment. I sent his stepfather over many times to see if he was alive when I couldn’t get in touch with him. I even called 911 on him when I thought he was suicidal, which resulted in a short hospital hold. I started to understand that he does not want this for himself, but doesn’t know how to stop. He fears withdrawal, and I hear his pain and cries when he begs me for money because he is so sick. He is eventually hospitalized for a blood infection. I realize I can no longer keep him in that apartment.
I clean the place out.
He didn’t need much food. The only thing in the fridge was water. I find all the things he has used as a tourniquet. There is an amazing amount of plastic garbage bag drawstrings removed from bags, Q-tips everywhere with the cotton taken off which are used as filters. So many water bottle caps. So many syringes.
“There were times I threw money into his car so angrily when he asked me. I struggled between loving him and hating him.”
I didn’t want my son to die, but I’m realizing I’m making it more comfortable for him.
Through most of his addiction he was highly functioning, always holding down a job. This was no longer the case.
He gets out of the hospital and is back to his car. I’m giving him $20 a day. He gets food stamps and Medicaid from the Department of Social Services. I find he sells what’s on his food stamp card. I pump gas in his car, but I do not hand over more cash. There were times I threw money in his car so angrily at him when he asked.
I struggled between loving him and hating him.
He began living in a hotel with his dealer and got arrested for possession of a syringe. He’s assigned a public defender, but of course Mom pays the fees and it’s knocked down.
But a few days prior, he made the choice on his own — which is key — to seek help.
He made the calls on his own, instead of me doing all of the legwork, to enter South Oaks Hospital in Amityville. His third try at rehab. But now, he wants it.
I went to a family meeting about 10 days in.
There he is. My son, my real son. Thank you, thank you and thank you.
He was enrolled in a 28-day program. He went to Mainstream House in Riverhead, a sober house. We do family things together again. We shop, we go to lunch, dinner. He wanted to be around us again. I haven’t had this in years. We laugh, we cry.
He got kicked out of sober living for having Ambien, a prescription drug, because he had a hard time sleeping. I let him back home. Kevin has a new job, a new girlfriend. He seems happy.
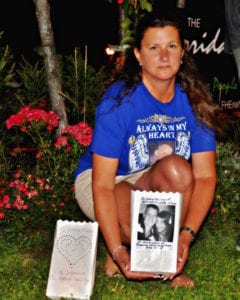
Tracey Farrell, a Rocky Point resident and founder of North Shore Drug Awareness Advocates, displays her luminaire in memory of her son Kevin Norris during the third annual Lights of Hope event in Port Jefferson on Aug. 31. Photo by Nora Milligan
I didn’t go to the classes I should have. I didn’t learn that someone new to recovery does not want their past thrown at them. One day at a time is their mantra. Yesterday is the past. He’s going to his meetings on a regular basis, but now that he is working, that starts to not be as often. Anything that goes missing I automatically accuse him. He wants a new phone because his is old and cracked. I bought him a new one and he “lost” it. I still tell him that if he didn’t sell it he would have it. He tells me he is working an honest program and that he has told me everything — including that he did not sell the phone. I apologize and tell him I am proud of him.
Kevin is working for a company which does party rentals.
One Sunday, in September 2012, he came home looking tired. He was thrilled that they gave him a $100 tip. They even gave him the leftover cake, which we of course ate together. We spoke of the cotton candy on his sneakers, because he worked the cotton candy machine. He thought it was fun.
The next day, his sister found him dead in bed. It was an accidental overdose.
They say money is a trigger.
I will never know what led him back. I know now I didn’t cause it. I couldn’t control it and I couldn’t cure it. I prepared myself that this day could come, but I thought he was in the clear. Our very last conversation was about cotton candy, one of the things I craved most when I was pregnant with him.
I still have the cotton-candy-covered shoe laces. I miss him every day. I still struggle with not doing the things I now know I should have done, and I try to teach people every day to not make the same mistakes I did. Learn from me please. Let me tell you anything and everything that may help you or your loved one. It helps me to help you.
I just went to a celebration meeting of one of his best friends celebrating one year of sobriety on Sunday, and he said, “I think he may have died so I can live.”
Tracey Farrell, formerly Tracey Budd, is a Rocky Point resident who, since her son’s passing, educates others on drug abuse and assists in finding help for those who are struggling, or know someone who is struggling, with addiction. She is the founder of North Shore Drug Awareness Advocates and also a 2015 TBR Person of the Year.
Commentators on the rising opioid crisis in the United States commonly say dealing with the problem requires a multi-pronged approach, and the Suffolk County Police Department agrees.
The department has expanded efforts to combat the many fronts of the opioid crisis, including prevention, treatment and enforcement.
Police Commissioner Tim Sini said in an interview that the opioid problem is the number one public safety and public health issue in Suffolk County.
“We have over 100 opioid-related overdoses every year for the past several years, and then when you consider the more than 500 Narcan saves on top of that, the tragic loss of life and the near tragic loss of life is just shocking,” he said at police headquarters in Yaphank.
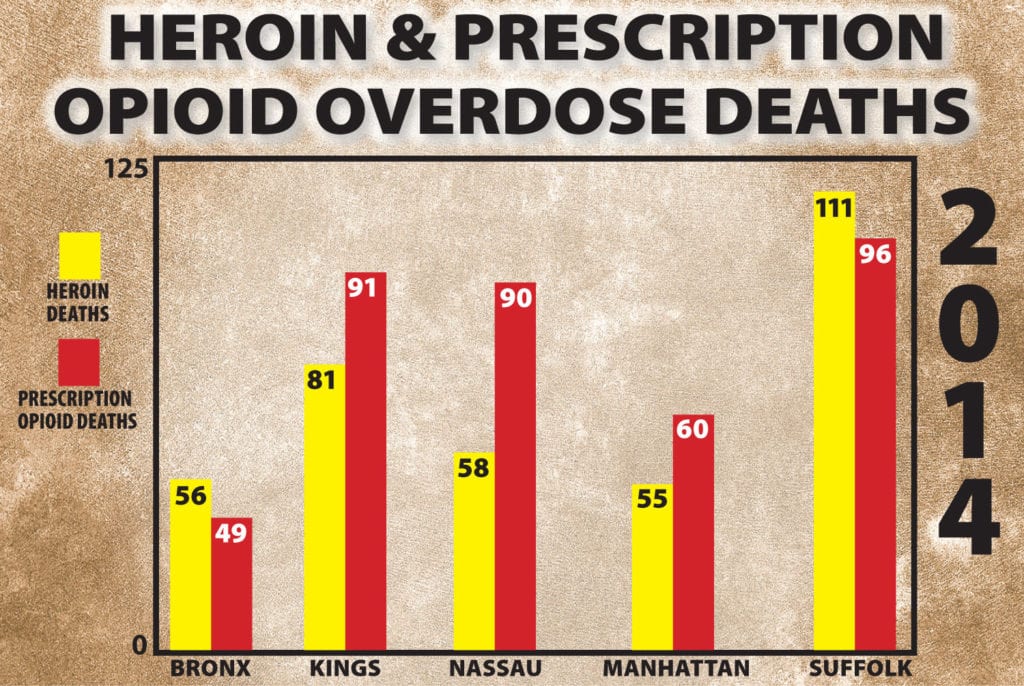
It’s no secret the SCPD has their job cut out for them — in 2014 Suffolk County had the highest number of overdose deaths involving heroin, and was the leader in deaths where prescription opioids were a factor in the state, according to a report by the New York State Comptroller’s office from June.
In 2014 Suffolk County had the highest number of overdose deaths with heroin, and was the leader in deaths where prescription opioids were a factor in NY
Sini also highlighted how crime is so closely associated with an increase in drug activity.
“Addicts often resort to burglaries and larcenies, and sometimes they elevate to robberies,” he said. “And now we’re seeing our gangs getting involved in the heroin trade because there is a lot of money to be made and there are so many customers.”
The commissioner said the department is working as hard as it can to ensure it’s as inconvenient as possible to sell drugs in Suffolk County.
At the end of March, SCPD started a program that encourages residents to call 631-852-NARC, an anonymous hotline encouraging residents to call in with drug tips they have. If the tip leads to an arrest, the resident is entitled to a cash reward. This initiative works in conjunction with Crime Stoppers, a program that connects local police departments with the public and media to help find suspects and collect information that can lead to arrests.
“Since we rolled [the drug hotline] out at the end of March, we’ve received over 500 tips on that line, and many of those have resulted in investigations and search warrants,” Sini said. “We’ve seized kilogram quantities of narcotics as a result of this initiative, over a million dollars in drug money, dozens and dozens of weapons, and over 200 arrests under this initiative. It’s important because not only does it take drugs off the street but it sends the message that we’re not going to tolerate drug dealing in our communities.”
The police department has said open communication with the public is an important part of this fight, because the more communities speak up and help the department, the better work the police can do.
Sini said since he took over, there has been almost a 200 percent increase in the amount of search warrants executed, and many of these are due to tips from residents.
“[Search warrants] are very important because it disrupts drug operations before they become too significant,” Sini said. “It takes guns and drugs off the streets, and also strengthens the partnership between the police department and the community. It encourages people to be more informative.”
Relationships with federal law enforcement partners have also been re-established, Sini said, and five detectives now work with the Drug Enforcement Administration; four focus on the heroin trade and the fifth investigates doctors and pharmacists who have been reported to unlawfully dispense or prescribe pain medication.
The police department has also focused resources on treating drug addicts who are in the throes of addiction.
Inmates at the Suffolk County Correctional Facility in Yaphank have the option of receiving voluntary medical assistance while still in jail. The department offers inmates who are eligible for the program, meaning they don’t have any drugs currently in their system and have said they want to commit to getting clean, an injection of Vivitrol, a drug that works as an opioid antagonist, blocking the opioid receptors in the brain and preventing someone from getting high for 30 days.
“It gives you that mental clarity and stability to essentially not relapse, so you can stay in treatment,” Sini said. “It’s highly effective but most addicts don’t want to use it because once you take that shot, you know you can’t get high for thirty days. So it takes someone who is really committed to getting help.”
Sini said the program starts in jail, and they look for inmates who have essentially been incarcerated because they are addicted to drugs, with arrests due to burglaries, possession, and other drug-related crimes. Incarcerated individuals receive their first shot in jail, and then are set up with a treatment provider in their community to work with when they are released.
“This is a multifaceted problem that creates issues for families, schools, the police department, probation, courts, medical examiners, churches and more. And everyone has got to be at the table.”
— Tim Sini
Suffolk County officers are also dedicated to providing programs that help with prevention.
The Ugly Truth is a program meant to educate school districts and community groups on the dangers this growing problem poses for all different age groups in Suffolk County. There are many other programs in effect right now being taught throughout the county.
“If we can prevent someone from ever going down that road, that’s where you’ll get your biggest bang for your buck,” Sini said.
The commissioner said he is only interested in working with evidence-based programs, which are resources that have been studied by analysts to prove their effectiveness.
Certain police officers are also designated as school resource officers. They are assigned to specific districts to participate in awareness programs with the students.
Sini said despite all the resources the department provides, more needs to be done.
“The silver lining is, among the experts there is consensus,” Sini said. “We don’t sit there and debate if addiction is a disease or if the cops can solve this problem. We all get it; this is a multifaceted problem that creates issues for families, schools, the police department, probation, courts, medical examiners, churches and more. And everyone has got to be at the table.”
Suffolk County leads New York State in deaths related to heroin and opioid overdoses. Graphic by TBR News Media
Suffolk County has a drug problem. And while it may be broken news, this is not breaking news.
Heroin and prescription opioid-related overdoses and deaths are increasing yearly across the nation, state and county, according to all available data, but the overall conversation lacks focus, those close to the issue have said. One Long Island man whose line of work leaves him with little insulation from the problem said it is worse than most would imagine.
Dan Moloney, who along with his brother Peter owns six Long Island locations of Moloney Family Funeral Homes, said in an exclusive interview that he believes the problem facing Suffolk County deserves a harsher spotlight. Moloney, who has an unenviable front row seat to the horrors that come from the addictive and powerful substance, said the problem reached a tipping point for him in 2009.
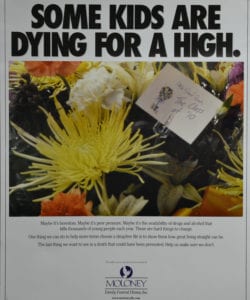
After a funeral for a Rocky Point student who overdosed, the Moloneys decided to try to use their platform to deliver an important message. They had posters made up with the words “Some kids are dying for a high” in bold letters on top of an image of a flower arrangement with a card that read, “With Deepest Sympathy, The class of ’10.” Below the image, the funeral director’s message read in part: “The last thing we want to see is a death that could have been prevented. Help us make sure we don’t.”
The Moloneys tried to distribute the posters to school districts around the Island, though they couldn’t find any takers.
Moloney’s Funeral home still has stacks of this poster. Photo by Alex Petroski
“Nobody wants to talk about it,” Dan Moloney said. “Nobody wants to hear from the funeral director.”
On the surface, in Suffolk County, it would appear heroin abuse is a daily conversation in one way or another, from politicians sponsoring initiatives to news outlets covering arrests and overdoses, to firsthand accounts from former addicts in various forms.
Moloney said he wouldn’t agree — not only is the problem receiving too little attention, he said, but also the wrong people are doing the talking.
“Are people sitting in the bleachers talking about the heroin problem?” he said. “But if their kid had some sort of disease, they’d be talking about it. They’d be doing fundraisers to help them find a cure.”
The two go hand-in-hand — heroin and opioids — or at least they should, Moloney said. Heroin is an illegal and highly addictive version of an opioid, according to the Centers for Disease Control and Prevention. However, statistics reporting deaths related to one or the other are not always paired.
The CDC’s website said health care providers wrote nearly a quarter of a billion prescriptions for legal opioids in 2013. Supply and demand for prescription pain medication doesn’t always dry up at the same rate. When the prescribed pills are gone and the desire for more lingers, the cheaper, stronger drug becomes a logical alternative.
In 2013, New York State’s Internet System for Tracking Over-Prescribing — Prescription Monitoring Program, also known as I-STOP/PMP, went into effect. The system works as a registry for practitioners to consult and track dispensed prescription histories for patients. The program has restricted supply of opioids to addicts, though it has done nothing to curb their demand. No tracking system exists for the neighborhood heroin dealer.
Moloney said one of his business’s facilities held funerals for three heroin overdose victims in just one day earlier this year. The closest comparison he could come up with to a public health concern inflicting that much damage in one day is a car crash that kills a vehicle full of people. He said that in some years, only two to three motorcycle-related deaths occur over the course of entire summer, which the public tends to find alarming, but that pales in comparison to heroin- and opioid-related deaths.
The difficulties in securing relevant and timely statistics on overdose-related deaths in New York State has contributed to undermining the understanding of the severity of Suffolk County’s problem, according to Moloney.
“Are people sitting in the bleachers talking about the heroin problem? But if their kid had some sort of disease, they’d be talking about it. They’d be doing fundraisers to help them find a cure.”
— Dan Maloney
“New York State is terrible,” he said about the state’s demographic record-keeping, which is an insight few could offer outside of the funeral business. “Three years down the road — the latest data you have is from three years ago. With the technology we have today, there’s absolutely no reason for that. And I know from colleagues that I have in other states, when you can’t get the information about how many deaths occurred in a certain place for two or three years, or what they were — because all of that is tracked — I just think the data that’s out there is antiquated and the situation is worse than the data they’re using shows.”
Father Francis Pizzarelli, director of Hope House Ministries in Port Jefferson, has been a regular contributor of insight and opinions regarding heroin and opioid addiction among young people in Suffolk County for about as long. He, like Moloney, said the problem is likely worse than anyone in the county realizes.
“The level of denial among parents continues to be deeply disturbing,” Pizzarelli wrote in a April 2016 column featured in this newspaper. Alcoholics Anonymous and Narcotics Anonymous, “which are a vital lifeline and network in our community for those working on recovery and wellness, have to worry that drug dealers are now waiting outside these meetings to prey on men and women in early recovery.”
Pizzarelli said his tipping point, much like that of Moloney’s, came in 2009. So far, though, he added, it has not been enough.
Suffolk County Police Commissioner Tim Sini said in May there were 103 fatal heroin overdoses in Suffolk County in 2015. New York State Comptroller Tom DiNapoli (D) released a report on June 9 saying there were more than 200 deaths in which heroin or opioids played a role in Suffolk County in 2014.
Regardless of how and when the deaths are identified with a specific cause or a contributing factor being opioids, one thing is clear to Moloney: the number is higher than we think.
According to the Suffolk County Police Department, since the act of administering the medication Narcan to reverse an opioid overdose became commonplace in August 2012, more than 630 saves have been recorded through Sept. 22.
In addition to conflicting stats, Moloney said an issue that he encounters is the stigma parents feel about losing a child to an overdose and what it might suggest about their aptitude as a parent. Most of the time, parents decline to immediately identify a heroin or opioid overdose as their child’s cause of death, he said. In fact, Moloney estimated that nine out of 10 parents whose child died of an overdose don’t address the issue and the cause isn’t added to a death certificate until about three months later, when lab reports are complete.
“It almost creates an environment where there doesn’t have to be an acknowledgement —not publicly,” Moloney said. “Of course there’s a lot of shame.”
Marisa Vitali, creator of “Grace,” speaks after the screening of the film. Photo by Victoria Espinoza
By Marisa Vitali
Life happens in the in-between spaces, from here to there. Recovery happens in the in-between spaces, when no one is looking and no one is around. How do we choose to live? How do we choose to be in those quiet moments with self? Have I filled my void, my spirit with happiness?
Or do I look outside myself for a drink, a drug, food, sex, shopping, cigarettes; to make myself not feel; to fill the void, the gaping black hole of low self-esteem and low self-worth?
I’ve learned that in recovery I have a choice. I’m no longer a slave to my next bag of dope and I can choose to see the glass half empty or half full.
Myself, I want it all, but when I logically prioritize, longevity and quality of life are on the top of the list. Every minute I spend obliterated is one less finite minute I have to feel life.
I do my best on a daily basis to choose happiness; to live happy, joyous and free. Recovery allows me to be in a place of rediscovery. To relearn the wisdom I was born with and somehow let slip between the fingers of my mind.
Just to be living is truly a gift and one not to be squandered on those people, places and things that cause us pain. Life is a gift to be celebrated and shared with those we love and who bring us even more joy than we may already be feeling.
Having this opportunity to live in recovery, I so know it didn’t have to be this way.
I always say: My life is nothing what I thought it would be and yet nothing I ever could have imagined it to be.
I don’t know the source of life, but I do know the humility I feel when confronted by nature and the magical way everything is prepared for every situation it could possibly encounter. That delusion in and of itself eliminates anxiety and I’m in deep.
I have come to the realization that living life to the fullest is not about my achievements — it is about my breath.
“I’ve learned that in recovery I have a choice. I’m no longer a slave to my next bag of dope and I can choose to see the glass half empty or half full.”
—Marisa Vitali
This moment, right here and now. Feeling everything there is to feel and experience in this one breath of in and out. This is what is intended. To soak in every drop of this thing called life.
We all intellectually know about breath and present moments so I will spare you the details in favor of encouraging you to do what you truly desire before it’s too late. Or keep collecting excuses that will serve you well in your final moments.
Because all we really have is today. There is no need to mar this experience with drugs and alcohol in order to escape this moment, this breath.
Not to make you nauseous with platitudes, but I do feel an urge to recap the classics. Living at the highest-level means feeling good about your life. There’s give and take without malice or greed, there is healthy socialization with challenging, stimulating people of integrity. There is reverence way before relevance, so if you turned down that road, I suggest you make a U-turn in the first driveway.
That’s what we’re all here for: to live the good, the bad and the ugly. To feel, to grow, to better ourselves and to help one another. We are here to serve, regardless of our elitist aspirations, so share your talents and energy freely. Our influence is exponential and will outlive us for eternity.
If one falls, we all fall, and so it’s a treasure and an opportunity to uplift one another in times of need with love, compassion and authenticity.
We all fall eventually. I fall at the door of a true friend. One of the most vivifying experiences is the exchange of love, and that I’m not afraid to express anymore.
This life, this recovery is a journey; it’s all in the same, with twists and turns, mountains and mole hills.
No matter what I choose not to use. I am evolving into whatever my imagination is capable of, without ego and defects of character that keep me small, dictating how it all should play out.
We are so much more powerful than we could possibly acknowledge. Tap into that source. Your source of creation, whatever that may be for you. The answers you seek are deep within.
There but for the grace of God go I. Live free, as the only thing constant is change.
So change! Do something different. I dare you. If nothing changes, nothing changes. Simple yet true.The clock is ticking. Seize the day and all that carpe diem s—.
But seriously, take a look around – this is all of your creation. You did this, you made this happen, you made these choices.
Will you run and hide like you’ve always done, or will you stand tall in the eye of the storm and dance in the rain?
We all have choices. I know what I choose. Do you? I dare you to live.
Marisa Vitali is a Northport native actress who created a short film about the journey of recovering from drug addiction.
Huntington town officials hope federal funding will help crack down on drug use and gang violence. File photo
State legislation
In the 2016 legislative session, Gov. Andrew Cuomo (D) signed a comprehensive package of bills, aimed at increasing access to treatment, expanding community prevention strategies and limiting the overprescription of opioids in the state. Some of the most important parts of the bills are highlighted below:
• Legislation now ensures insurers must cover “necessary” inpatient services for substance use disorder treatments for as long as an individual needs them. Review from the company can only begin 14 days after treatment to ensure each patient has two weeks of uninterrupted and covered care.
• Insurers are prohibited from requiring prior approval for emergency supplies of these medications.
• Insurers must use objective state-approved criteria to determine the level of care for individuals suffering from substance abuse.
• Insurers must cover the costs of Narcan to families with individuals suffering from substance abuse.
• Families now offered 72 hours of emergency treatment, instead of 48 hours, for family members so they can be stabilized and connected to longer-term addiction treatment options while also balancing individual rights of the incapacitated individuals.
• Requires hospitals to provide follow-up service options to individuals upon hospital discharge to connect patients with nearby treatment options to provide continuous medical care.
• Reducing opioid prescription limits from 30 days to seven days, with exceptions of chronic pain and other conditions.
• Health care professionals must complete three hours of education every three years on addiction, pain management and palliative care.
State budget
The 2016-17 state government has allotted funding to help curb the growing substance abuse problem. A breakdown of the budget below:
• Nearly $200 million through the New York State Office of Alcoholism and Substance Abuse Services will be used to combat the heroin and opioid epidemic, an 82 percent increase in state spending since 2011.
• This investment includes $66 million for residential treatment beds, including counseling and support services for roughly 8,000 individuals.
• $38 million to fund medication-assisted treatment programs that serve about 12,000 clients in residential or outpatient settings.
• $25 million in funding for state-operated addiction treatment centers.
• $24 million for outpatient services that provide group and individual counseling.
• $8 million for crisis/detox programs to manage and treat withdrawal from heroin and opioids.
NYS Heroin and Opioid Task Force
Comprised of health care providers, policy advocates, educators, parents and New Yorkers in recovery, the task force will build on the state’s previous efforts and use its expertise and first-hand experience to develop a comprehensive action plan to combat the state’s opioid epidemic. The task force will focus immediately on expanding awareness of heroin and opioid addiction; enhance statewide prevention efforts; increase access to treatment; improve support for those in recovery; and concentrate on law enforcement recommendations to reduce the supply of opioids. Members plan to hold public sessions across the state.
Comprehensive Addiction and Recovery Act, 2016
• Signed into law by President Barack Obama (D) in July.
• $8.3 billion in addiction funding.
• $160 million for the expansion of medication-assisted treatment options, including grants that will be awarded to state, local and tribal governments to provide opioid abuse services.
• $80 million in funding to help prevent and treat addiction on a local level through community-based education, prevention, treatment and recovery programs.
• $103 million to establish a community-based competitive grant program to address and treat the problems of heroin and opioid addiction and abuse.
• Grants will help fund programs that could expand treatment alternatives to incarcerations — with consent of attorneys and participants — for individuals who meet the program’s criteria.