Can we overcome our genes?
By David Dunaief, M.D.

We have made great strides in the fight against heart disease, yet it remains the number one cause of death in the United States. Approximately one-third of Americans over the age of 35 will die of heart disease (1). I hope this statistic has captured your attention, because it should. What is causing or contributing to such high numbers of heart disease deaths: genetics, environment or both? Many of us have the propensity toward heart disease. Can we alter this course, or is it our destiny?
A 2013 study, involving the Paleo-type diet and other ancient diets, suggests that there is a significant genetic component to cardiovascular disease, while another study looking at the Mediterranean-type diet implies that we may be able to reduce risk factors greatly. Most of the risk factors for heart disease, such as high blood pressure, high cholesterol, sedentary lifestyle, diabetes, smoking and obesity are modifiable (2). Let’s look at the evidence.
Genetic components
In a study published online in The Lancet, researchers used computed tomography scans to look at 137 mummies from ancient times across the world, including Egypt, Peru, the Aleutian Islands and Southwestern America (3). The cultures were diverse, including hunter-gatherers (consumers of a Paleo-type diet), farmer-gatherers and solely farmers. Their diets were not vegetarian but rather involved significant amounts of animal protein: fish and/or cattle.
Researchers found that one-third of these mummies had atherosclerosis (plaques in the arteries), which is a precursor to heart disease. The ratio should sound familiar. It seems to coordinate with modern times.
Interestingly, but not surprisingly, the average age of death was 43. The authors concluded that atherosclerosis could be part of the aging process in humans. In other words, it may be a result of our genes. Being human, we all have a genetic propensity toward atherosclerosis and heart disease — some more than others — but many of us can reduce our risk factors significantly.
I am not saying that the Paleo-type diet specifically is not beneficial compared to the standard American diet. Rather, that we do not know it based on this study, which was not meant to provide the validity of the Paleo-type diet, but whether atherosclerosis is part of the normal aging process. However, other studies demonstrate that we can reduce our chances of getting heart disease with lifestyle changes, potentially by following a Mediterranean-type diet with an emphasis on a plant-rich approach.
Mediterranean-type diet
A study about the Mediterranean-type diet and its potential positive impact on cardiovascular disease risk was published in the New England Journal of Medicine (4). Here, two variations on the Mediterranean-type diet were compared to a low-fat diet. People were randomly assigned to three different groups. The two Mediterranean-type diet groups both showed about a 30 percent reduction in the risk of cardiovascular disease, with end points including heart attacks, strokes and mortality, compared to the low-fat diet. This improvement in risk profile occurred even though there was no significant weight loss.
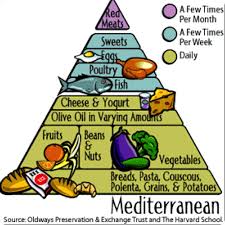
The Mediterranean-type diets both consisted of significant amounts of fruits, vegetables, nuts, beans, fish, olive oil and potentially wine. I call them “the Mediterranean diet with opulence,” because both groups consuming this diet had either significant amount of nuts or olive oil and/or wine. If the participants in the Mediterranean diet groups drank wine, they were encouraged to drink at least one glass a day.
The study included three groups: a Mediterranean diet supplemented with mixed nuts (almonds, hazelnuts or walnuts), a Mediterranean diet supplemented with extra virgin olive oil (at least four tablespoons a day) and a low-fat control diet. The patient population included over 7,000 participants in Spain at high risk for cardiovascular disease. The high-risk population included those with high blood pressure (80 percent of the population), diabetes and those who were overweight and/or were smokers.
The strength of this study, beyond its high-risk population and its large size, was that it was a randomized clinical trial, the gold standard of trials. However, there was a significant flaw, and the results need to be tempered. The group assigned to the low-fat diet was not, in fact, able to maintain this diet throughout the study. Therefore, it really became a comparison between variations on the Mediterranean diet and the standard American diet.
What do the leaders in the field of cardiovascular disease and integrative medicine think of the Mediterranean diet study? Interestingly there are two diametrically opposed opinions, split by field. You may be surprised by which group liked it and which did not. Cardiologists hailed the study as a great achievement. They included Henry Black, M.D., who specializes in high blood pressure, and Eric Topol, M.D. They emphasized that now there is a large RCT measuring clinical outcomes, such as heart attacks, stroke and death.
On the other hand, the integrative medicine physicians, Caldwell Esselstyn, M.D., and Dean Ornish, M.D., both of whom stress a plant-rich diet that may be significantly more nutrient dense than the Mediterranean diet in the study, expressed disappointment with the results. They feel that heart disease and its risk factors can be reversed, not just reduced. Both clinicians have published small, well-designed studies showing significant benefits from plant-based diets (5, 6). Ornish actually showed a reversal of atherosclerosis in one of his studies (7).
So which group of physicians is correct about the Mediterranean diet? Each opinion has its merits. The cardiologists’ enthusiasm is warranted, because a Mediterranean diet, even one of “opulence,” will appeal to more participants, who will then realize the benefits. However, those who follow a more strict diet, with greater amounts of nutrient-dense foods, will potentially see a reversal in heart disease, minimizing risk — and not just reducing it.
Thus, even with a genetic proclivity toward cardiovascular disease, we can very much alter our destinies. The degree depends on the willingness of the participants. Potentially, we can have an impact that ranges from reduction to reversal.
References: (1) Circulation. 2008;117(4):e25. (2) www.uptodate.com. (3) The Lancet. 2013;Mar 11. (4) N Engl J Med. Online 2013;Feb 25. (5) J Fam Pract. 1995;41(6):560-568. (6) Am J Cardiol. 2011;108:498-507. (7) JAMA. 1998 Dec 16;280(23):2001-2007.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.