
Ministrokes are not inconsequential
By David Dunaief, M.D.

A TIA (transient ischemic attack) is sometimes referred to as a ministroke. This is a disservice since it makes a TIA sound like something that should be taken lightly. Ischemia is reduced or blocked blood flow to the tissue, due to a clot or narrowing of the arteries. Symptoms may last less than five minutes. However, a TIA is a warning shot across the bow that needs to be taken very seriously on its own merit. It may portend life-threatening or debilitating complications that can be prevented with a combination of medications and lifestyle modifications.
Is TIA common?
It is diagnosed in anywhere from 200,000 to 500,000 Americans each year (1). The operative word is “diagnosed,” because it is considered to be significantly underdiagnosed. I have helped manage patients with symptoms as understated as the onset of double vision. Other symptoms may include facial or limb weakness on one side, slurred speech or problems comprehending others, dizziness or difficulty balancing or blindness in one or both eyes (2). TIA incidence increases with age (3).
What is a TIA?
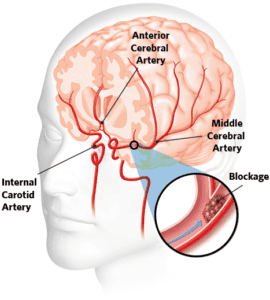
The definition has changed over time from one purely based on time (less than one hour), to differentiate it from a stroke, to one that is tissue based. It is a brief episode of neurological dysfunction caused by focal brain ischemia or retinal ischemia (low blood flow in the back of the eye) without evidence of acute infarction (tissue death) (4). In other words, TIA has a rapid onset with potential to cause temporary muscle weakness, creating difficulty in activities such as walking, speaking and swallowing, as well as dizziness and double vision.
Why take a TIA seriously if its debilitating effects are temporary?
Though they are temporary, TIAs have potential complications, from increased risk of stroke to heightened depressive risk to even death. Despite the seriousness of TIAs, patients or caregivers often delay receiving treatment.
Stroke risk
After a TIA, stroke risk goes up dramatically. Even within the first 24 hours, stroke risk can be 5 percent (5). According to one study, the incidence of stroke is 11 percent after seven days, which means that almost one in 10 people will experience a stroke after a TIA (6). Even worse, over the long term, the probability that a patient will experience a stroke reaches approximately 30 percent, one in three, after five years (7).
To go even further, there was a study that looked at the immediacy of treatment. The EXPRESS study, a population-based study that considered the effect of urgent treatment of TIA and minor stroke on recurrent stroke, evaluated 1,287 patients, comparing their initial treatment times after experiencing a TIA or minor stroke and their subsequent outcomes (8).
The Phase 1 cohort was assessed within a median of three days of symptoms and received a first prescription within 20 days. In Phase 2, median delays for assessment and first prescription were less than one day. All patients were followed for two years after treatment. Phase 2 patients had significantly improved outcomes over the Phase 1 patients. Ninety-day stroke risk was reduced from 10 to 2 percent, an 80 percent improvement.
The study’s authors advocate for the creation of TIA clinics that are equipped to diagnose and treat TIA patients to increase the likelihood of early evaluation and treatment and decrease the likelihood of a stroke within 90 days. The moral of the story is: Treat a TIA as a stroke should be treated, the faster the diagnosis and treatment, the lower the likelihood of sequela, or complications.
Predicting the risk of stroke complications
Both DWI (diffusion weighted imaging) and ABCD2 are potentially valuable predictors of stroke after TIA. The ABCD2 is a clinical tool used by physicians. ABCD2 stands for Age, Blood pressure, Clinical features and Diabetes, and it uses a scoring system from 0 to 7 to predict the risk of a stroke within the first two days of a TIA (9).
Heart attack
In one epidemiological study, the incidence of a heart attack after a TIA increased by 200 percent (10). These were patients without known heart disease. Interestingly, the risk of heart attacks was much higher in those over 60 years of age and continued for years after the event. Just because you may not have had a heart attack within three months after a TIA, this is an insidious effect; the average time frame for patients was five years from TIA to heart attack. Even patients taking statins to lower cholesterol were at higher risk of heart attack after a TIA.
Mortality
If stroke and heart attack were not enough, TIAs decrease overall survival by 4 percent after one year, by 13 percent after five years and by 20 percent after nine years, especially in those over age 65, according to a study published in Stroke (11). The reason younger patients had a better survival rate, the authors surmise, is that their comorbidity (additional diseases) profile was more favorable.
Depression
In a cohort (particular group of patients) study that involved over 5,000 participants, TIA was associated with an almost 2.5-times increased risk of depressive disorder (12). Those who had multiple TIAs had a higher likelihood of depressive disorder. Unlike with stroke, in TIA it takes much longer to diagnose depression, about three years after the event.
What can you do?
Awareness and education are important. While 67 percent of stroke patients receive education about their condition, only 35 percent of TIA patients do (13). Many risk factors are potentially modifiable, with high blood pressure being at the top of the list, as well as high cholesterol, increasing age (over 55) and diabetes.
Secondary prevention (preventing recurrence) and prevention of complications are similar to those of stroke protocols. Medications may include aspirin, antiplatelets and anticoagulants. Lifestyle modifications include a Mediterranean and DASH diet combination. Patients should not start an aspirin regimen for chronic preventive use without the guidance of a physician.
In researching information for this article, I realized that there are not many separate studies for TIA; they are usually clumped with stroke studies. This underscores the seriousness of this malady. If you or someone you know has TIA symptoms, the patient needs to see a neurologist and a primary care physician and/or a cardiologist immediately for assessment and treatment to reduce risk of stroke and other long-term effects.
References:
(1) Stroke. Apr 2005;36(4):720-723; Neurology. May 13 2003;60(9):1429-1434. (2) mayoclinic.org. (3) Stroke. Apr 2005;36(4):720-723. (4) N Engl J Med. Nov 21 2002;347(21):1713-1716. (5) Neurology. 2011 Sept 27; 77:1222. (6) Lancet Neurol. Dec 2007;6(12):1063-1072. (7) Albers et al., 1999. (8) Stroke. 2008;39:2400-2401. (9) Lancet. 2007;9558;398:283-292. (10) Stroke. 2011; 42:935-940. (11) Stroke. 2012 Jan;43(1):79-85. (12) Stroke. 2011 Jul;42(7):1857-1861. (13) JAMA. 2005 Mar 23;293(12):1435.
Dr. Dunaief is a speaker, author and local lifestyle medicine physician focusing on the integration of medicine, nutrition, fitness and stress management. For further information, visit www.medicalcompassmd.com or consult your personal physician.


